Anatomy def: Puke is an English word meaning to vomit or to expunge the gastric contents.
Outlander def: Jamie’s sea voyage compulsion to hurl his first wife’s ginger tea or anything else residing in his wobbly wame! Ralph, heave, upchuck, spew, gag, be sick, retch, barf, throw up, regurgitate, emit, and disgorge – we all ken the vicious urgency of a tummy that demands purging!!!
BTW, have you assumed the word, puke, is a 20th century invention? Or, have ye ever wondered who invented such a poetic term?
Well, none other than “The Bard,” Himself! Puke first appeared in Shakespeare’s As You Like It (II. vii. 144):
At first the infant, mewling, and puking in the nurse’s arms,”…
Who knew?
Read about Jamie’s “Battle of the Wame” in Diana’s splendid tome, Voyager! if you haven’t read these marvelous stories, hope you get “on board” soon (hah!).
“Never mind,” I said. I glared back over my shoulder at the heap of reeking bedclothes. It stirred slightly, and a groping hand emerged, patting gingerly around the floor until it found the basin that stood there. Grasping this, the hand disappeared into the murky depths of the berth, from which presently emerged the sound of dry retching.
See Jamie’s agonizing heave hos in Starz ep 309, The Doldrums.His wretched retching caused my own wame to wobble a wee bit! How ’bout you? ?
Hey, anatomy students! Great to see you again. Today’s lesson slides further along the GI tract’s slippery slope, as we visit the stomach. The stomach goes by a mess of nicknames: abdomen, beer belly, belly, breadbasket, girth, gut, guts, insides, middle, paunch, pot, potbelly, spare tire, tummy, and Jamie’s fav, the wame! Most of these terms actually refer to the anterior abdominal wall (Anatomy Lesson #16, “Jamie’s Belly” or “Scottish Six-Pack”), a cause of anguish for many of us (Image A). But, for anatomists, stomach or gaster (Greek gastēr meaning stomach) specifies an organ of the GI tract.
The stomach is absolutely fascinating and near and dear to my heart as in the 80’s and 90’s it was the focus of my research; during that time, I published 100+ papers, abstracts, and invited lecturers in far flung places such as Holland and Japan. Although a few papers ventured into realms of liver and colon, most focussed on stomach. So, let’s have a meet-and-greet with the stupendous stomach. Outlander images included for free (psst, they are near lesson’s end)!
Image A
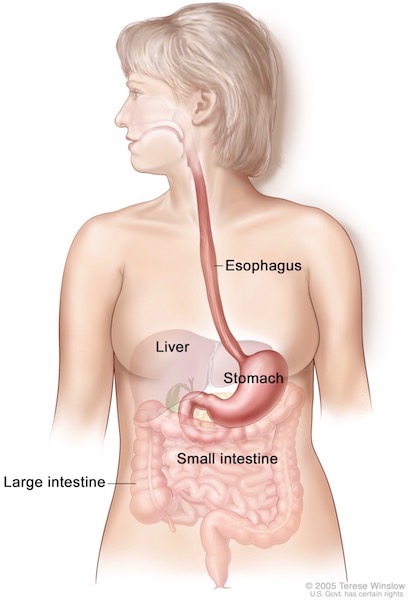
Stomach: The stomach is a hollow, dilated, comma-shaped organ of the GI tract, dwelling between esophagus (Anatomy Lesson #45, “GI System – Part 2”) and duodenum (first part of small intestine). Tucked under the respiratory diaphragm, it sits in the upper left abdominal cavity (Image B).
Image B
Stomach Relationships: Centrally placed, the stomach contacts many other organs, a fact relevant to the spread of some cancers. These organs are:
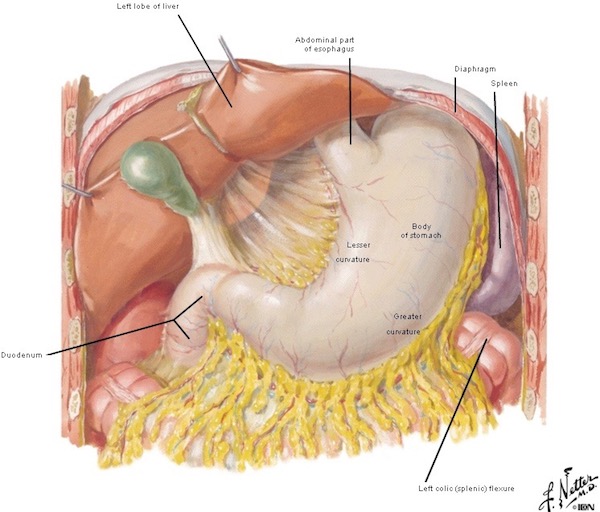
Understand that due to embryology, the stomach lies on it’s side (Image C) exposing two curves: the lesser curvature faces to our right and the greater curvature faces to our left.
Image C
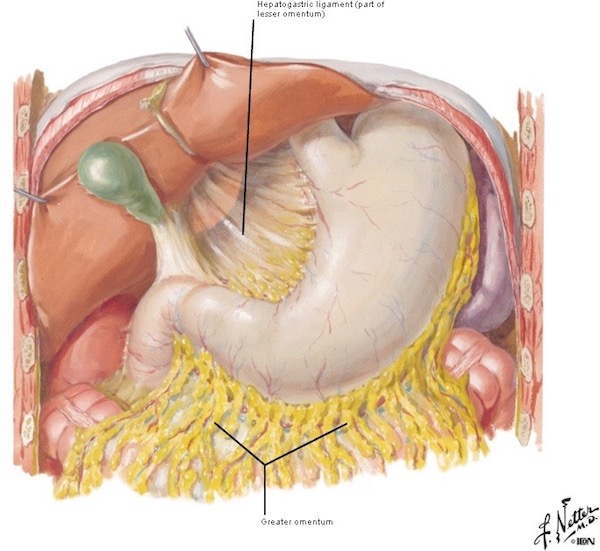
Stomach Mesenteries: The stomach doesn’t drift in the abdominal cavity, rather, it is anchored by mesenteries, double layers of peritoneum, a membrane lining the abdominal cavity and covering most of its organs (Image D). Mesenteries are challenging to explain without a lesson of gut embryology, but, such structures suspend stomach from spleen, diaphragm, colon, and liver.
The lesser omentum (obscure Latin origin) is a mesentery connecting lesser curvature of stomach with liver.
The larger, greater omentum hangs from the greater curvature of the stomach, draping over the intestines much like an apron. It is the first structure encountered when the abdominal cavity is opened via anterior incision. The greater omentum serves as a storage depot containing various amounts of adipose (fat) tissue. It also houses pockets of macrophages, a type of white cell that ingests debris, foreign material, microbes, etc. Amazingly, the greater omentum also wraps around and isolates areas of infection, foreign bodies, or trauma, walling them off from other abdominal organs!
Image D
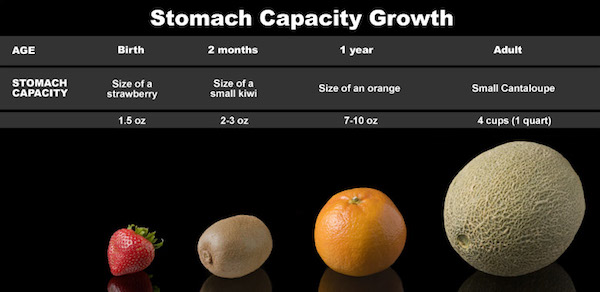
Stomach Capacity: The stomach is a hollow bag which expands to accommodate a meal. The gastric capacity changes from the size of a strawberry in newborns to the size of a small cantaloupe in adults (Image E). Thus, a normal adult stomach has the capacity of about 1 liter (1+ qt.). Once an adult, stomach capacity stays pretty constant. If we stuff ourselves during the holidays, It can expand to 5x its normal size, but it returns to its former size once the food has gone bye-bye. The Internet is filled with claims about dieting, purging, stuffing, stomach size, etc. Here are a few myths about the stomach:
Stomach Myth #1: Eating less food shrinks the stomach. It doesn’t. Eating less won’t shrink the stomach, but it does reset the hunger thermostat (in the brain) so we don’t crave as much food to feel full.
Stomach Myth #2: Skinny people have smaller stomachs than heavier people. They don’t. A person’s weight doesn’t determine stomach size.
Stomach Myth #3: Dieting shrinks the stomach. It doesn’t. An adult stomach remains the same size although dieting can rid one of belly fat both internally and under the belly skin.
Image E
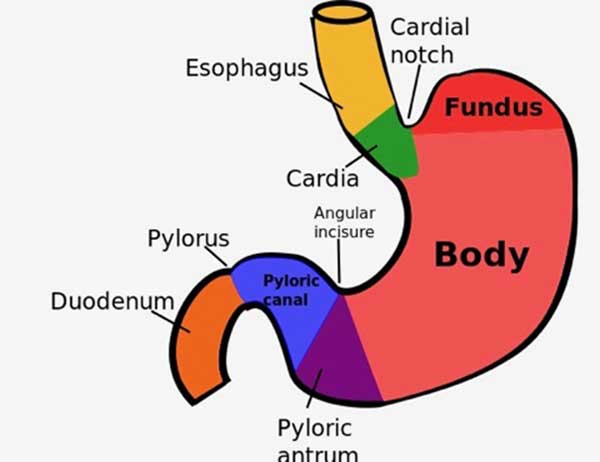
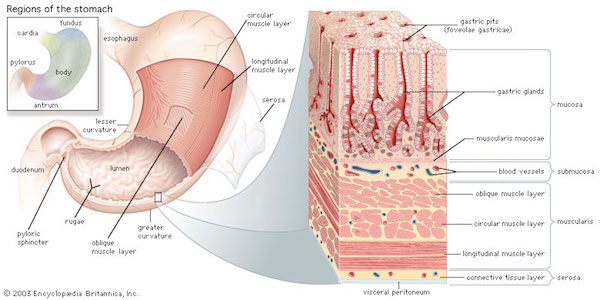
Stomach Parts: Anatomists could not leave well enough alone, sigh, they had to divide the stomach into regions (Image F). Why? Because they have anatomical and physiological differences:
cardia (green), region adjoining the esophagus
fundus (red), upper curvature of stomach. From the Latin meaning bottom – go figure!
body (dark pink) main, middle part of stomach
pyloric antrum (purple) is the lower part of the stomach
pyloric canal (blue) tubular area of stomach which empties into the duodenum (orange).
pyoric sphincter terminal valve leading into duodenum (labelled pylorus)
Image F
Now, let’s examine the thick stomach wall, endowed with muscle and mucosa (and other stuff that you won’t find compelling so we’ll skip them).
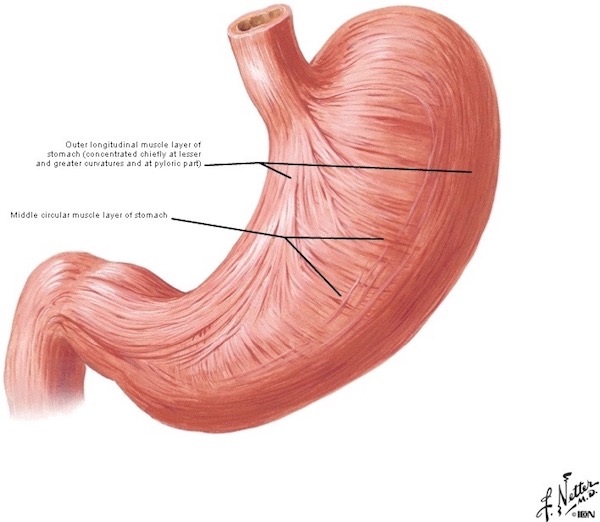
Stomach Muscle: The stomach wall is thickened with layers of smooth muscle. You remember smooth muscle from Anatomy Lesson #45? This type lacks cross striations and is under autonomic (involuntary) control.
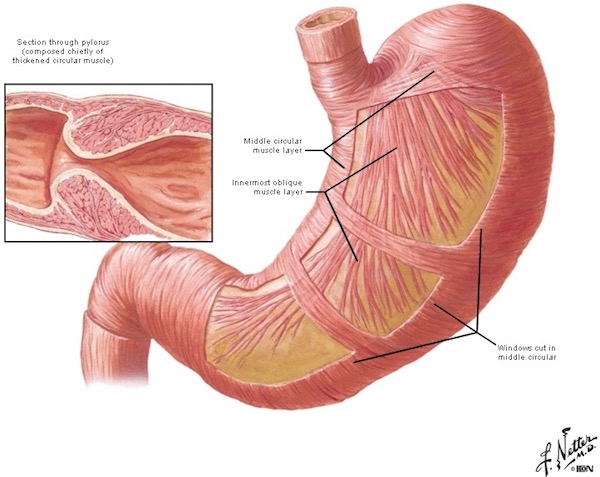
The stomach wall is endowed with three thick layers of smooth muscle oriented in different axes. The outer longitudinal layer of smooth muscle is oriented with the long axis of the stomach. A middle layer of smooth muscle encircles the lumen (Image G).
Image G
An innermost oblique smooth muscle layer is oriented at angles to both longitudinal and circular layers. At the pylorus, the circular layer thickens markedly to form the pyloric sphincter, which contracts to retain gastric contents or relaxes to allow the contents to enter the duodenum (Image H).
Such muscle layers aren’t just another pretty face; in fact, contraction of these layers serve a very important function, discuss below.
Image H
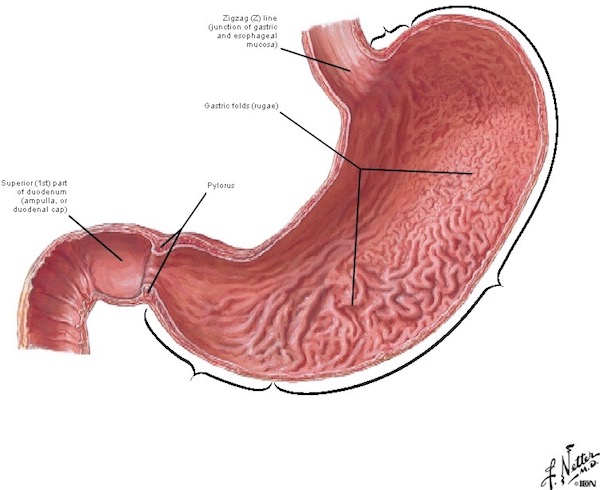
Gastric Rugae: Opening the stomach along its long axis reveals the lumen (central space) and lining mucosa. Last lesson, we learned the mucosa is a layer of living cells lining a lumen. Internally, the landscape is not smooth, rather it is thrown into numerous rugae, folds of the gastric mucosa (Image I).
The purpose of rugae are two fold: they stretch outward and flatten, allowing the stomach to expand and accommodate food and drink and they increase surface area for absorption. Note the zig-zag (Z) line marking the gastroesophageal junction at the gastric entrance – we learned about it in the last lesson (Anatomy Lesson #45, “Tremendous Tube – GI System, Part 2”). The pyloris marks the far end of the stomach – more about it soon.
Image I
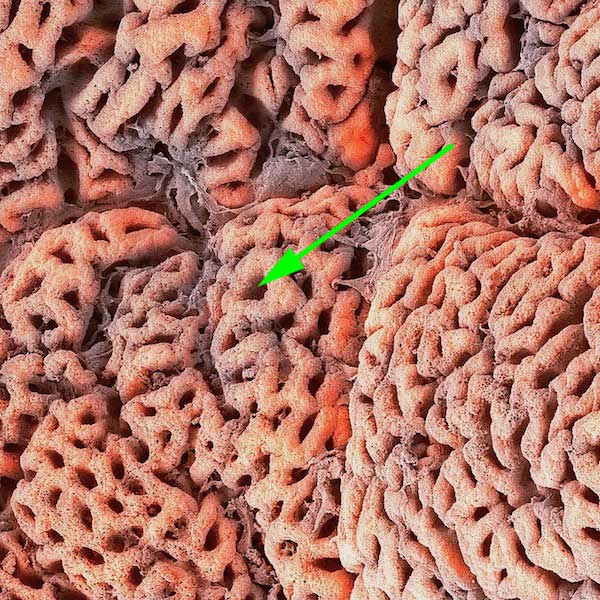
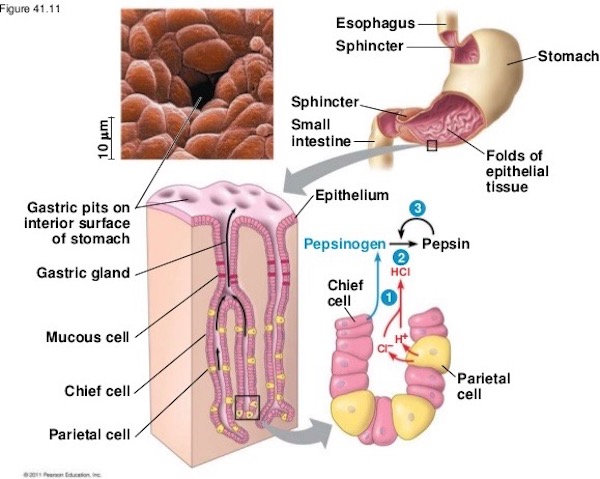
Gastric Pits: If you stand inside your gastric lumen (not recommended, <G>), you certainly will see the rugae. But, let’s say you zoom in and view the mucosal surface using a scanning electron microscope (SEM) (Anatomy Lesson #34, “The Amazing Saga of Human Anatomy”); you would behold an amazing site-sight! The entire surface of the gastric mucosa is dimpled with holes known as gastric pits (Image J – green arrow). Gastric pits plunge down into the mucosa much like open water wells into the ground.
Surface mucosal cells (bumps) surround the holes. When stimulated, these cells produce mucus and bicarbonate (think baking soda). BTW, the orange color is computer generated, not natural.
Image J – Photo by Steve Gschmeissner gastric pits
Gastric glands: One or more gastric glands open into the base of each pit, so glandular secretions flow up the gastric pits and into the gastric lumen. The stomach has millions of pits and multimillions of glands. Got it? Swell! Now, these glands contain different cell populations depending on their location. Thus, the fundus and body contain gastric glands; the pylorus contains pyloric glands (Image K). Oh, and dinna worry about all the layers listed in Image K; these are for folks taking histology/microscopic anatomy courses.
Image K
Now, don’t let Image L scare you away just because it shows a little physiology (lower right)! Hang on and let me explain….. upper left of the image is an SEM of the mouth of a single gastric pit. The bumps surrounding it are surface mucosal cells. Below it is a diagram showing two gastric glands opening into the base of one gastric pit; let’s focus on this part of the diagram.
Gastric glands contain several different cell types. One type (mucous cell) produces mucus, another type (chief cell) produces pepsinogen/pepsin, a protein-cleaving enzyme, and lipase, an enzyme that metabolizes fats. Gastric glands also contain APUD cells (not labelled) which produce several hormone-like substances controlling stomach, gallbladder and small intestine activity. And, then, we have the parietal cell – ta da!
Image L
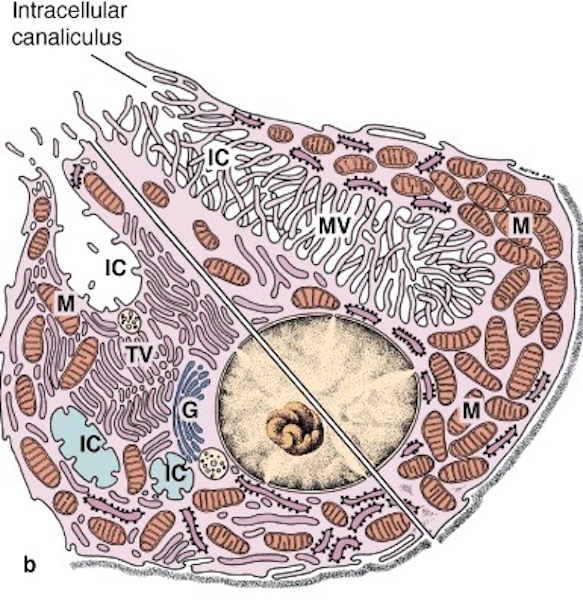
Parietal Cell: Parietal cells are powerful, period! They deserve super special recognition because they produce hydrochloric acid (HCl), a gastric acid of pH ∼1.5 (pH measures acidity or alkalinity) – almost as acidic as battery acid! This harrowing stuff is necessary to denature (unravel) dietary proteins so they can be digested. It also destroys microbes in our food and drink. Even with a clean kitchen, our food is loaded with bacteria. Scrub brush, STAT!
Here’s a quickie of how parietal cells produce HCl. Each cell can change its shape as shown in Image M, a split drawing. When a parietal cell is resting (Image M – bottom half of cell), it has a tiny inlet (labelled IC) extending a short way into the cell. When parietal cells are stimulated (image M – top half of cell), the inlet or bay (intracellular canaliculus) expands dramatically and HCl ions (components) are pumped across the cell membrane and into the IC; they flow up the gastric pit and into the gastric lumen.
Needing more to do, pariental cells also produce intrinsic factor (IF), a glycoprotein required to absorb Vitamin B12. One may consume all the B12 in the world, but none can be absorbed without intrinsic factor. Lacking intrinsic factor and B12, our brains and nervous systems function poorly and we cannot form normal red blood cells (Anatomy Lesson #37, “Outlander Owies Part 3 – Mars and Scars”). So, take a big bow, parietal cell – we thank ye kindly!
In summary, parietal, mucous, APUD and chief cells generated fluids that pour into the gastric lumen after food is received from the esophagus. The powerful muscular wall then contracts in waves mixing food and fluids into a watery mass known as chyme.
Image M
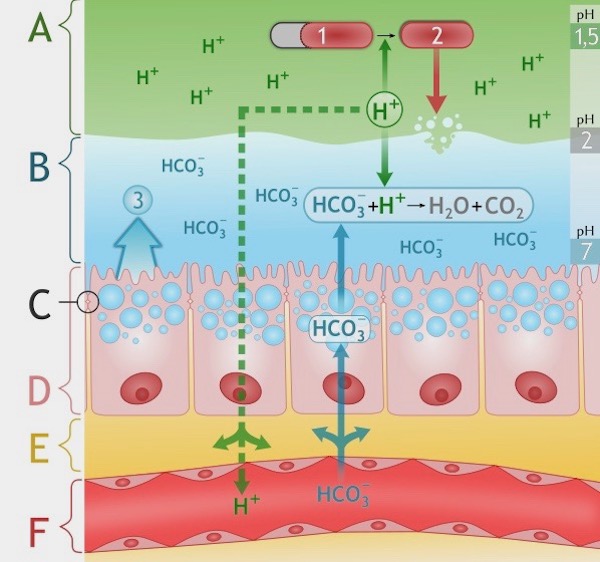
Gastric Mucosal Barrier: Now, being curious anatomy students, you must wonder how the stomach withstands gastric juices nearly as caustic as battery acid??? Of course, you do! Well, it is complex. Decades ago, this protective feature was termed the gastric mucosal barrier (GMB), although no one knew exactly what it was.
After more than 30 years of effort and millions of research dollars, it appears that the GMB isn’t one protective mechanism, it is at least three: tight junctions, mucus, and bicarbonate!
Tight Junctions: Surface mucosal cells are “joined at the hip” by tight junctions; unions so tight, they exclude harsh gastric fluids.
Mucus: A layer of insoluble mucus tenaciously clings to the surface mucosal cells forming a barrier against auto-digestion by pepsin and erosion by HCl.
Bicarbonate: When parietal cells release HCl, surface mucosal cells release a tide of bicarbonate (think baking soda, again) to neutralize nearby gastric acid.
These three factors conspire to bring the pH near the surface mucosal cells to 7 or neutral…neither acidic or alkaline (Image N)!
Layer A is gastric acid, pH 1.5. Über caustic!
Layer B is insoluble mucus and bicarbonate (HCO3-) released by surface mucosal cells (pH 2-7)
Layer C is the union of tight junctions (see circle – very tiny) joining surface mucosal cells (pH 7)
Layer D is the surface mucosal cell layer
(p.s. Let’s ignore layers E and F)
Ergo, the stomach creates a harsh luminal environment and the GMB protects the stomach from its own offspring!
Image N
Historical Tidbit: A hundred years before Jamie’s time, European scientists argued about the purpose of the human stomach. Some claimed the it was a stove wherein food literally burned. Others sided with Galen, declaring it a storehouse that sorted wheat from chaff. Still others posited the stomach was a fermentation vat. BTW, the vat idea wasn’t confined to Europe as it also appears in 19th century Japanee wood blocks prints. Image O shows the artist’s concept of a good diet. A vat representing the stomach complete with attendants appears in the upper left abdominal quadrant. So, whose argument was correct?
Image O by Inshoku Yōjō, Kagami Kabuki wood blocks
This who’s “right – fight” continued for another century until John Hunter arrived on the scene (Anatomy Lesson #3, “Bad Day at Cocknammon Rock” or “Wee Bonny Fingers on my Collar Bone!”). Diana wrote about Hunter in her 7th book (Image P) – hope you read it! Dr. Hunter (1728-1793) aptly responded to the debate: “Some physiologists will have it that the stomach is a mill, others that it is a fermenting vat, but a stomach, gentlemen, is a stomach.“ Reminds me of Sigmund Freud’s supposed comment about his omnipresent “sexualized” cigar: “Gentlemen, sometimes a cigar is just a cigar!”
Image P Oil painting after Sir Joshua Reynolds.
Now, onto the pylorus.
Pylorus: (How to pronounce this word? Pylorus rhymes with Delores. Har, har! (Those who follow Diana may get this wee joke.) Pylorus is a Greek word meaning gatekeeper. Why the name? Because the pyloric sphincter opens in controlled waves allowing small “gulps” of chyme into the duodenum. Too much chyme, too quickly, and one is greeted with nausea, vomiting, cramping, bloating, and diarrhea! This activity is highly controlled.
In a nutshell, we now know the splendid stomach gives us the follow splendid gifts:
Acid: secrets HCl to denature ingested proteins and kill bacteria.
Pepsin and lipase: releases enzymes to digest proteins and fats.
Churn: smooth muscle layers contract in waves to mix food, mucus and HCl into watery chyme.
Hormones: secretes six hormone-like substances controlling stomach, small intestine, and gallbladder.
Informant: senses carbohydrates, proteins, and fats and informs the brain to evaluate food palatability and link nutritional value with taste.
Storage: stores chyme until hormones and nerves signal the pyloric sphincter to relax.
Absorption: takes up water, aspirin, ethanol, caffeine, water soluble vitamins and alcohol, etc.!
Alcohol: Speaking of alcohol, the gastric mucosa (and liver) contains alcohol dehydrogenase, an enzyme which detoxifies alcohol at the rate of roughly one stiff drink per hour. On average, men have more of this enzyme than women and, thus, can metabolize alcohol more effectively. Sorry gals, this isn’t sexist, it is nature! (Take comfort, there are things gals do better than guys). Looks like mighty fine wine (Starz, episode 204, La Dame Blanche). You, Jamie, not the drink. Snort!
Alcohol: Because the stomach absorbs alcohol, this is an apropos spot to insert the topic of alcohol and pregnancy. Some fans have asked about Claire’s drinking alcohol while pregnant with Faith (Starz episode 204, La Dame Blanche). Today, we are well aware that pregnant women must avoid the perils of alcohol, but given the time and place of Outlander S.2, drinking by pregnant women would have been prevalent. Fetal alcohol syndrome even wasn’t described until 1973, well after Claire’s pregnancies, so even as a battle-trained nurse, she would have been unaware of it’s detrimental effects. Thanks production team for staying true to the times depicted. Go Outlander team. Rah!
Now, does the knowledge that alcohol ingestion can adversely effect a pregnancy stop some women from imbibing? Consider a statement by Brit Henry Youngman: “When I read about the dangers of drinking, I gave up reading.” Human logic can take one to very odd places!
Vomiting: Gah, even the word sounds ominous! This awful bodily reaction occurs as the stomach seeks to purge itself of noxious stuff. Vomiting goes by many names: ralph (where did that name come from?), heave, upchuck, spew, gag, be sick, retch, barf (my fav), puke, throw up, regurgitate, emit, and disgorge!
Vomiting comes in two phases. First, during the retching phase, abdominal, thoracic, and diaphragmatic muscles undergo convulsive contractions (you know the drill) but nothing is expelled. Second, during the expulsion phase, retrograde peristalsis starts in the small intestine and sweeps upwards. Pyloric and lower esophageal sphincters relax. Thoracic and abdominal muscles contract to increased intra-thoracic and intra-abdominal pressures which propel gastric contents upwards to explode all over Aunt Jocasta’s Isfahan carpet! Mop, STAT!
Retching is preceded by feelings of nausea and increased salivation, deep breaths, sweating, and increased heart rate. You ken, right? These responses are helpful as salivation helps protect tooth enamel from stomach acids (very corrosive). The deep breath helps prevent aspirating vomit into the larynx. Sweating and increased heart rate are autonomic responses to stress.
No Persian carpet at the abbey, but Claire feels nauseous for sure (Starz episode 116, To Ransom A Man’s Soul)! Her look of distress, a sheen of sweat, plus the belly grip is a sure signal that her wame is wobbly. Of course, Murtagh and the Monk (good book title? <g>) haven’t a clue that the lass is pregnant – they think she swoons because beloved Jamie lies depressed, damaged, and despairing! Well, that, too.
Now, nausea and vomiting are common among pregnant women. Only about 30% of expectant moms are spared either or both. But, Claire isn’t one of the lucky ones. Her’s is a willful, wobbly wame. She barely gets Jamie’s hand repaired before losing her parritch behind a colum, oops, column, in the abbey corridor (Starz episode 116, To Ransom A Man’s Soul). I know, I know, it’s a lame joke, but we must keep spirits up while we wait, wait, and WAIT for S.3!
Even after arriving in Paris, Claire continues upchucking. Herself explains, from Dragonfly in Amber book:
“No. I’m quite all right now.” And I was. In the odd way of morning sickness, once the inexorable nausea had had its way with me, I felt perfectly fine within a moment or two. “Let me just rinse my mouth.”
…“Sassenach, you’re with child! Ye dinna mean to go out to nurse beggars and criminals?” … I pressed my hands against my belly, squinting down. “It isn’t really noticeable yet; with a loose gown I can get away with it for a time. And there’s nothing wrong with me except the morning sickness; no reason why I shouldn’t work for some months yet.”
…“Feeling all right, are ye, Sassenach? The sickness is better?” “Much.” The morning sickness had in fact abated, though waves of nausea still assailed me at odd moments.
Claire’s vomiting at the abbey had au naturale causes. But, in Paris, poison is the culprit! Well, truth be told, Comte St. Germain is the blackguard as he conspires to poison her drink (Starz, episode 204, La Dame Blanche). Gloating, he doesn’t give a fig about her or her unborn child. Let them eat cake!
Next day, Claire hikes up to Master Raymond’s apothecary (Starz, episode 204, La Dame Blanche): “I was violently ill last night. Someone tried to kill me. I almost died!”
But, the Master kindly informs his fav madonna: “The effect is most immediate… The stomach seeks to purge itself and, well, you get the idea.” The Master sells bitter cascara to clients (think Comte servant) who in a moment of passion, seek to poison their enemy. But, while the enemy visibly suffers (to the satisfaction of the poisoner), it doesn’t kill them (to the satisfaction of the poisoned).
Diana offers more insight, from Dragonfly in Amber book:
“Poison for a rival,” he said. “Or at least she thinks so.” “Oh?” I said. “And what is it really? Bitter cascara?” He looked at me in pleased surprise. “You’re very good at this,” he said. “A natural talent, or were you taught? Well, no matter.” He waved a broad palm, dismissing the matter. “Yes, that’s right, cascara. The rival will fall sick tomorrow, suffer visibly in order to satisfy the Vicomtesse’s desire for revenge and convince her that her purchase was a good one, and then she will recover, with no permanent harm done, and the Vicomtesse will attribute the recovery to the intervention of the priest or a counterspell done by a sorcerer employed by the victim.”
Just so you know, bitter cascara was a folk medicine historically used as a laxative by native Americans and American immigrants. The plant was not identified by scientists until the 1800s, although its European counterpart (European buckthorn) appeared in a 17th century London Pharmacopoeia. Today, it is unavailable in US laxatives because of harmful side effects including intestinal pain, severe diarrhea with dehydration, and abortive action. That is to say…. avoid!
Stomach Diseases: At least 11 diseases commonly plague the stomach. Since we cannot cover all, let’s “talk” about ghastly gastric ulcers.
For decades, doctors thought stress, spicy foods, smoking, or other lifestyle habits caused peptic ulcers. But, in 1982, two Australian physicians, Drs. Marshall and Warren, reported a link between Helicobacter pylori and gastritis/gastric ulcers (for which each received a Nobel Prize!). Many in the medical community found the report heretical as it was believed no bacterium could survive the acidic gastric environment. Facing steep criticism, Dr. Marshall courageously drank a culture of H. pylori and within three days developed gastritis. Yep, cause and effect. Surprised by his dedication? Think Claire – tasting urine for sugar content at L’Hôpital des Anges!
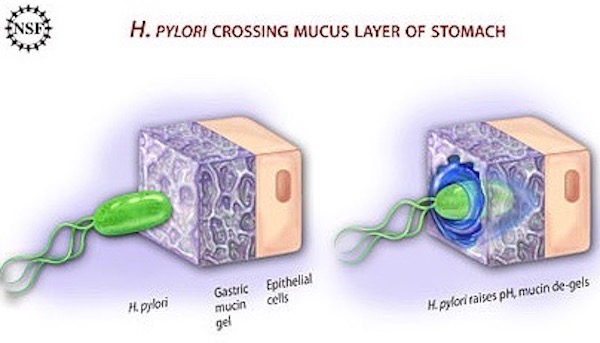
Helicobacter Pylori:
H. pylori is shaped like a corkscrew with flagella (motile tails). Burrowing through the mucous layer, it creates ammonia which damages and destroys surface mucosal cells (Image Q). The hole in the mucous layer also allows luminal HCl to contact surface mucosal cells, adding to the damage and leading to gastritis and/or ulcers (talk about biting the hand that feeds you!). Ulcers are serious complications as they can bleed, cause infection, or even block the passage of food in the digestive tract. Not good!
Hard to believe, but world-wide, 50% of all humans carry H. pyloris! For unknown reasons, most carriers are asymptomatic and infections are treatable with antibiotics. Whew!
Image Q
Let’s end this anatomy lesson with another splendid stomach story from an earlier era! In 1822, William Beaumont, a 27 y.o. surgeon in the U.S. Army, was stationed at Ft. MacKinac, Michigan. One fine day, Alexis St. Martin, an employee of the American Fur Company, was brought to his surgery. Martin had been shot in the back by accidental discharge from a musket less than a yard away. Yep, shooting accidents happened well before our time!
The wound was the size of a man’s hand and included fractured ribs, lacerated diaphragm, torn left lung, and a perforated stomach! The dirty wound contained remnants of musket discharge, pieces of clothing, and shards of rib, all of which were driven into the chest cavity. The exit wound, under the left breast, included some stomach extruding the remnants of a recent meal. Och! Dr. Beaumont pushed lung and stomach back into proper position and treated the wound with a fermenting poultice, ammonia, and vinegar followed with oral aqueous camphor. The next day, he bled Alexis (unfortunate, but true to the times), and gave an oral cathartic which promptly “escaped from the stomach through the wound.”
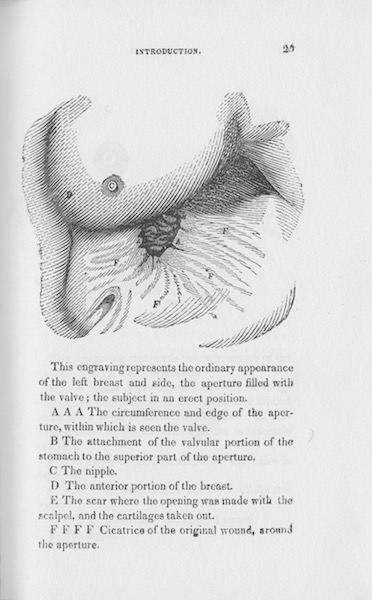
Dr. Beaumont fully expected Alexis to die. This did not happen, but something amazing did! Alexis’ wound healed (sans antibiotics) leaving a fistula (abnormal connection) between the stomach and his skin (Image R). Understand that Alexis had a strong constitution and lived to be 60 y.o.! A drawing of his healed wound appears in Image R.
Image R
Alexis’ wound produced a “window” into the gastric lumen. Now, very little was known about the stomach at that time, so Beaumont launched a series of gastric experiments (1825 -1833). During this time, Dr. Bill devised clever experiments wherein he observed changes of the gastric mucosa during fasting, eating, and drinking. He tied string to chunks of food and lower them through the fistula. He then observed and recorded changes in the stomach as it responded to each morsel. He also tapped gastric juice and described its activities outside the body (Image S) and he recorded the effects of various alcohols on the gastric mucosa.
Image S
Dr. Beaumont meticulously recorded his observations over the next eight years! Then in 1833, with his own funds, and never having published before, he published his own book: “Experiments and Observations on the Gastric Juice and the Physiology of Digestion” (Image T). To this day, his observations and conclusions have not been refuted (amazing!). His reward for this effort? Today, he is known as the “Father of gastric physiology.” But, one of the most amazing details of this story… Dr. Beaumont never went to medical school (he apprenticed)!
Speaking of observations and conclusions: Claire would have respected Dr. Beaumont’s devotion to the scientific method unlike her withering opinion of Gillian Edgar’s (Geillis Duncan) “scientific method.” Here, from Dragonfly in Amber book:
In a parody of the scientific method, the first section of the book was titled “Observations.” It contained disjointed references, tidy drawings, and carefully numbered tables.
And below, the notebook filled with fine cursive script, laying out in strict order conclusion and delusion, mingling myth and science, drawing from learned men and legends, all of it based on the power of dreams. To any casual observer, it could be either a muddle of half-thought-out nonsense or, at best, the outline for a clever-silly novel. Only to me did it have the look of a careful, deliberate plan.
The central section of the notebook was titled “Speculations.” That was accurate, at least, I reflected wryly.
Back to Beaumont and St. Martin! I am honored to own a facsimile of Dr. Beaumont’s book, one of the most prized in my anatomy library. I hope you can muster a bit of awe for this accomplishment. Today, such experiments would be deemed unethical, but remember the times – this helps me keep such events in perspective.
Image T
Woo hoo, prof! The bell has rung and time to stop. We ken ye adore the stomach, but do bring this lesson to a close. It’s almost Christmas Eve! Hee, hee.
”The stomach is lowest and has a hidden place in the body because of its uncleanness, as though nature had spared the principal members and had relegated the stomach or bowels farther away from the site of reason and of the mind and fenced it off with the diaphragm in order not to disturb the rational part of the mind with its importunity. These members serve the higher ones. Some of them concoct the food into juice, others digest it into various humors, others expel the superfluity.” — Alessandro Benedetti, 1497
WRONG! I once worked with a pair of colleagues who shared Alessandro’s opinion, mocking the stomach as lowly and insignificant. Over the years, attitudes have shifted to those of considerable respect for the superb, spectacular, sumptuous, sublime and splendid stomach. It has “convos” with the brain, folks! <G>
Now, as Starz hasn’t graced us with an image of the anatomical stomach, will this one do (Starz, episode 204, La Dame Blanche)? Snort! Hike that sark up a wee bit more, Jamie, no a better wame anywhere. Double snort!
“Up on the housetop reindeer paws…..” Santa? Naw, it’s just the Bonny One with a nasty monkey bite. Hah!