
A sublime blend of beauty and belligerence…tomorrow, July 21st, in Anatomy Lesson #26: “Jamie’s Chin – Manly Mentus.”
The deeply grateful,
Outlander Anatomist

Human Anatomy taught through the lens of the Outlander books by Diana Gabaldon and the Starz television series
A sublime blend of beauty and belligerence…tomorrow, July 21st, in Anatomy Lesson #26: “Jamie’s Chin – Manly Mentus.”
The deeply grateful,
Outlander Anatomist
Summertime greetings to all Outlander anatomy students! Anatomy Lesson #24 covered the outer ear so today’s Anatomy Lesson #25 is the Ear – Part 2, or to be more exacting the middle and inner ears.
But first, what does a tree have to do with the ear? The title of this lesson derives from a 300 year old philosophical thought: “If a tree falls in a forest and no one is around to hear it, does it make a sound?” An 1884 issue of Scientific American correctly addressed this question. What do you think? Watch for the answer later on!
And to emphasize the importance of the ear in society, do you ken that the English language is replete with many idioms of all things ear? One website lists 120+ idioms including: a tin ear, all ears, music to the ears, up to the ears in, wet behind the ears, bend one’s ears, can’t make a silk purse out of a sow’s ear (who would try?), cute as a bugs ear (didn’t know bugs had ‘em), fall on deaf ears, in one ear and out the other, turn a deaf ear, and blow it out your ear (here’s to you, BJR!).
Now, onto the lesson. To review, in anatomy lesson #24 we learned that the human ear is divided into three ears: an outer (Photo A- green), a middle (Photo A- yellow) and an inner ear (Photo A- blue). That lesson dwelt almost exclusively on the outer ear. So, now we move to the middle and inner ears.
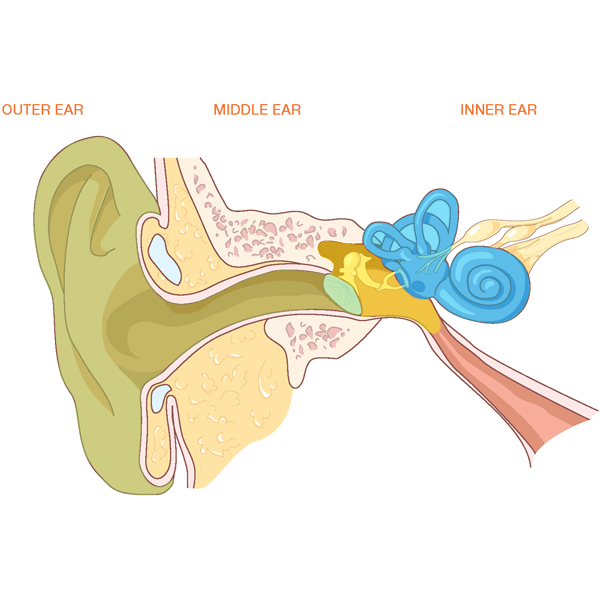
Photo A
Let’s begin with the middle ears. Each middle ear is housed inside a cavity within one of our two temporal bones. The human skull includes 22 bones two of which are os temporale (Latin meaning temporal bone). The temporal bone is weirdly shaped (Photo B – pink bone). From a side view, it comprises most of the skull around the external acoustic meatus or EAM (Anatomy Lesson #24). The temporal bone also includes the zygomatic arch, part of the cheek bone (Anatomy Lesson # 8) and the gothic-looking styloid process marked by the black arrow (Anatomy Lesson #12). Let’s add a new part of the temporal bone which is pertinent to today’s lesson, the rounded mastoid process.
Try this: Place your fingers behind the pinna of one ear and move downward until you feel a rounded mound of bone; this is your mastoid process. It typically lies just below the level of the EAM or ear hole as Claire called it (ha ha). Its outer layer is compact bone, but inside it is riddled with air-filled spaces. Well done folks!
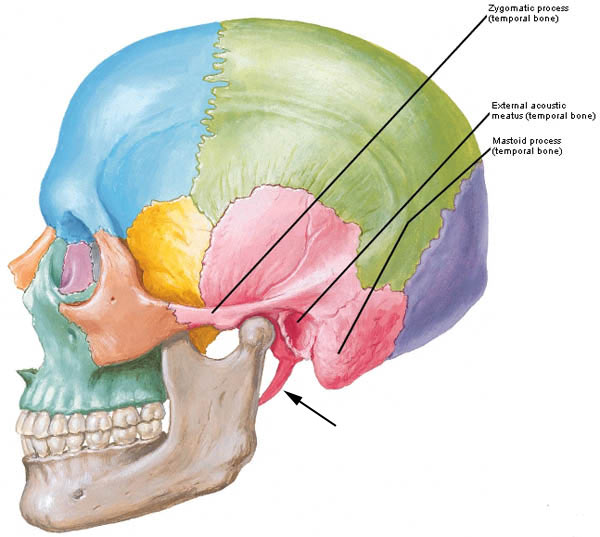
Photo B
A different image of the skull helps us appreciate the location of the middle ear. With the top of the skull and brain removed, Photo C shows the cranial base. The right side of the image shows the tortuous shape of the bony floor upon which the brain rests. Nerves and blood vessels pass through the many holes in the skull bones. The left side of the image is color coded so once again, the temporal bone is pink. See the bright green area? This is the location of the middle ear – it lies inside the petrous (Latin meaning stone-like) part of the temporal bone, one of the densest bones of the human body.
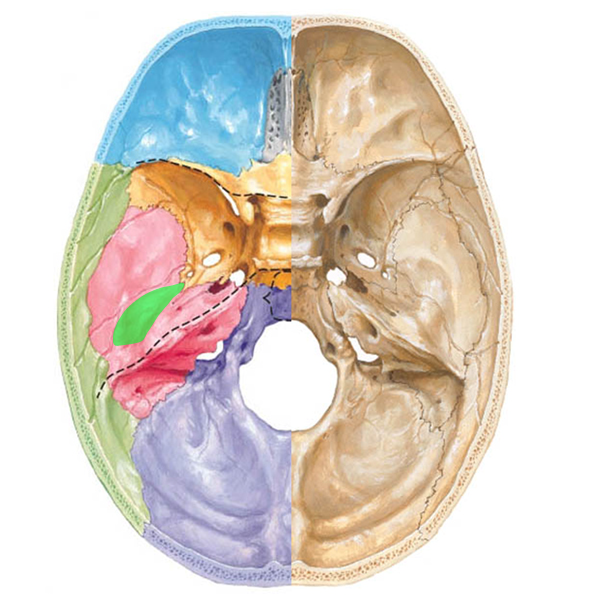
Photo C
The middle ear is small but it contains a large number of components including tympanic cavity, inner leaflet of tympanic membrane, three bones, the opening of a throat tube, a posterior “attic door,” two wee windows, two tiny muscles, a nerve and a nerve plexus. Wow! That’s quite a list for such a small space! Let’s examine the components.
The tympanic cavity is an air-filled chamber (Photo D, yellow dashed line) inside the petrous temporal bone; its shape is so difficult to describe that many anatomists compare it to a small room with four walls, a roof and floor. So let’s do that: the roof and floor are petrous temporal bone. The outer (lateral) wall is the tympanic membrane. The inner (medial) wall will be discussed shortly. The back wall has an “attic door” leading to the mastoid air cells (see below). The front wall receives the opening of the throat tube or pharyngotympanic or Eustachian tube (photo D) that extends between the back of the throat and the tympanic cavity.
Please understand this: normally, air pressure between the tympanic cavity and the EAM is equal. However, as we climb in altitude, air pressure becomes lower in the EAM than in the tympanic cavity which pushes the tympanic membrane outward causing discomfort, even pain. As we descend in altitude, air pressure is higher in the EAM than in the tympanic cavity which pushes the tympanic membrane inward, again causing pain. Air pressure equalizes on each side of the tympanic membrane when we open the Eustachian tubes: with altitude, air escapes from the tympanic cavity and with descent, air enters the tympanic cavity. Got it? Chewing and swallowing activates a pair of itsy, bitsy, teeny weeny, tensor veli palatini muscles that open the Eustachian tubes to equalize the air pressure. I won’t show an image of these wee muscles because it will clutter the lesson. Just know that they work well unless the Eustachian tubes are congested.
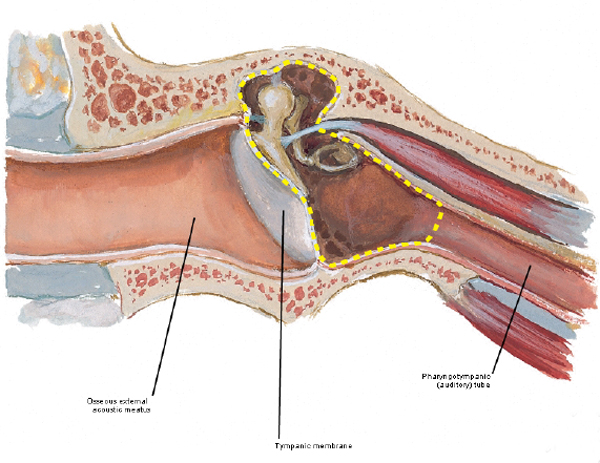
Photo D
Remember the “attic door” in the back wall of the tympanic cavity? It has a longish Latin name, the aditus ad antrum, but the short of it is that the passageway leads to air cells which riddle the mastoid process (Photo E). These little spaces are thought to reduce the mass of the skull bones and provide physical protection.
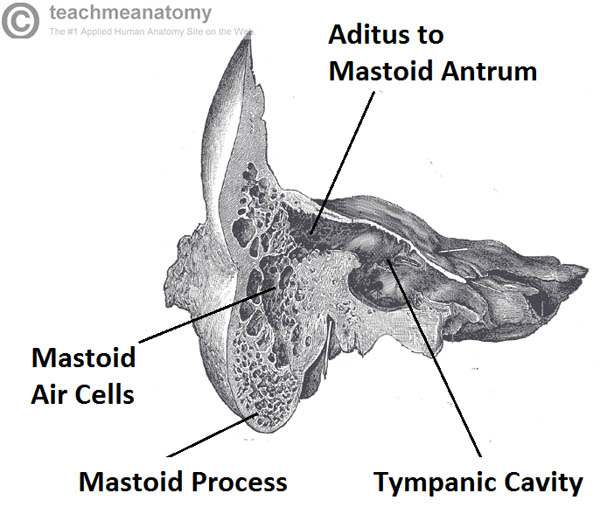
Photo E
The middle ear bones bring us back to the anatomical rule of three! Three ossicles meaning tiny bones are the smallest bones of the human body. How small are they? Well, all three easily fit on a U.S. dime with plenty of wiggle room (Photo F)! There are three ossicles per middle ear and they are not included in the count of 22 skull bones.

Photo F
The ossicles form a tortuous bridge spanning the tympanic cavity from outer to inner walls (Photo G). Each ossicle resembles the object for which it is named: the malleus (Latin meaning hammer) has a handle firmly attached to the inner leaflet of the tympanic membrane and a head that articulates (forms a joint with) the incus. The incus (Latin meaning anvil) articulates with the stapes (Latin meaning stirrup) and the stapes inserts into the oval window, an opening in the inner wall of the tympanic cavity. Although tiny, the joints or articulations between the ossicles are moveable.
Please understand this: imagination is sometimes required to relate the Latin names to their corresponding anatomical objects. However, ancient anatomists used objects found in nature to name the body parts. The names such as stapes or malleus seem quaint but I actually prefer them to the current naming trend which often includes meaningless words containing lots of “cs”, “xs” and “zs.”
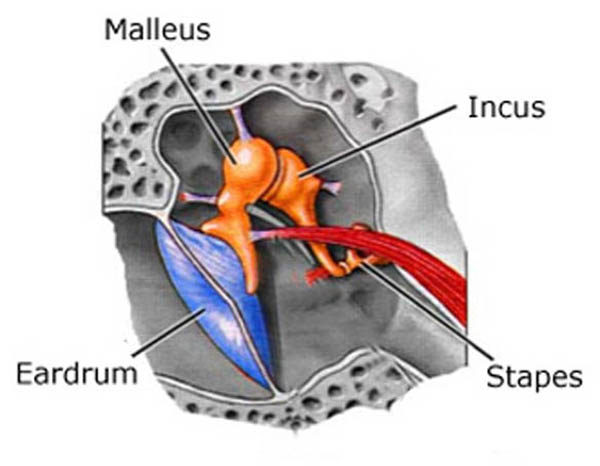
Photo G
The inner wall of the tympanic membrane bears two holes piercing the temporal bone. One hole, the oval window, is plugged by the stapes (Photo H); the other hole or round window is closed by a membrane (Photo H – black arrow). The inner wall has several other features too, but these are beyond the scope of this lesson
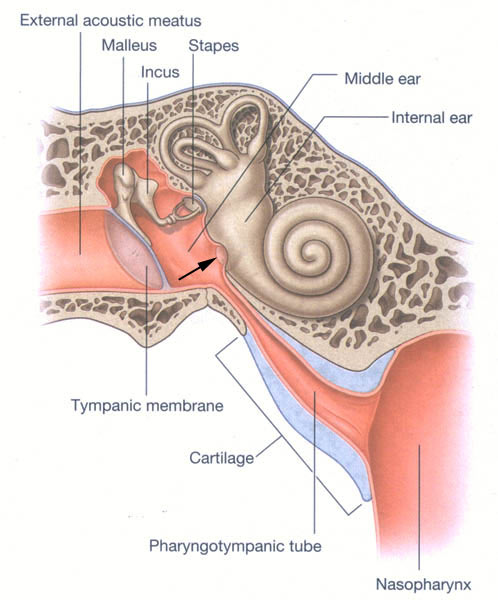
Photo H
Let’s stop for a short Clinical Correlation: The oral cavity and throat contain oodles of bacteria (Rupert and Angus consider germs in this hilarious video: Angus and Rupert Go Through The Stones). All is well unless they follow the Eustachian tube into the tympanic cavity where they can set up housekeeping to our detriment. Otitis media (Latin meaning inflammation of middle ear) is a rather common condition which typically includes bacterial (or viral) infections of the middle ear. Over 30 million doctor visits per year in the U.S. are due to otitis media. Symptoms include: pain, pulling at the pinna, irritability, sleeplessness, crying, etc. A trip to the doctor and an otoscope exam is in order (Photo I).

Photo I
Anatomy Lesson #24, showed the photo of a normal tympanic membrane (Photo J – left). But, with otitis media, the tympanic membrane is red, bulging because there is fluid in the middle ear and it hurts (Photo J – right)! Proper treatment is imperative.

Photo J
Unresolved otitis media can lead to mastoiditis (Latin meaning inflammation of mastoid bone). Now, dinna confuse mastoiditis with mastitis which is inflammation of the breast. Och, we are discussing ears, not mammary glands!
Here’s how mastoiditis works: recall that little attic door in the back wall of the middle ear that leads to the mastoid air cells (photo E)? Well, that door is a perfect conduit for bacteria to make their way from the middle ear into the mastoid air cells causing serious health complications in children and adults. Photo K (left side) shows bacterial invasion of the mastoid air cells and its presentation at the body surface (Photo K – right side). Signs include fever, redness, swelling, and tenderness behind the pinna which is pushed outward and forward.
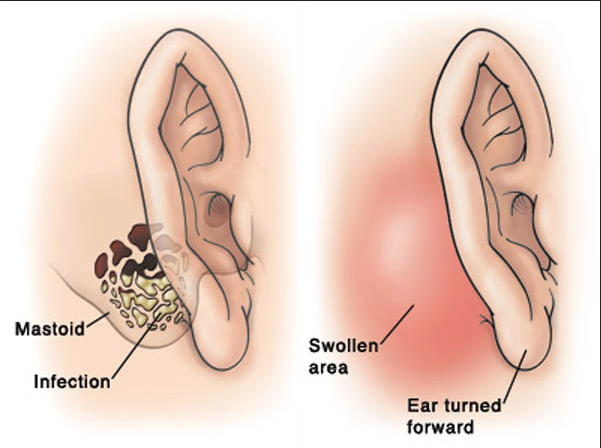
Photo K
A picture is worth a thousand words, so this photo shows a case of mastoiditis (photo L – left mastoid process). Ouch, that hurts!

Photo L
Now back to anatomy. The inner ear is the last and by far the most complex of the three “ears”. At first blush it resembles a mutant squid or snail. It contains both bony and membranous elements. Bony parts include cochlea, vestibule and three (yes, three!) semicircular canals (Photo M- tan structures) filled with fluid (perilymph). Membranous elements (Photo M – blue structures) are suspended within the bony parts; these are the cochlear duct, utricle, saccule and three semicircular ducts; these are surrounded by perilymph and are filled with endolymph. Only the cochlear duct is involved in hearing, the utricle, saccule and semicircular ducts are necessary for balance and equilibrium.
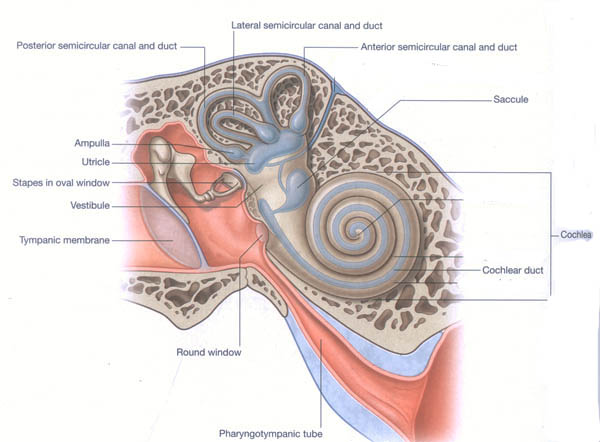
Photo M
The cochlea and its cochlear duct spiral 2.5 times much like a snail shell. Within each cochlear duct lies the organ of Corti, a strip of 15,000-18,000 specialized “hair” cells arranged in rows like soldiers. “Bristles” project from the surfaces of the “hair” cells although these are unlike the hairs of skin. When examined by scanning electron microscopy (Anatomy Lesson #6), the bristles resemble the pipes of an organ (Photo N – cat hair cells). The bristles are covered by a gelatinous membrane (not shown in Photo N). The organ of Corti is also our organ of hearing.
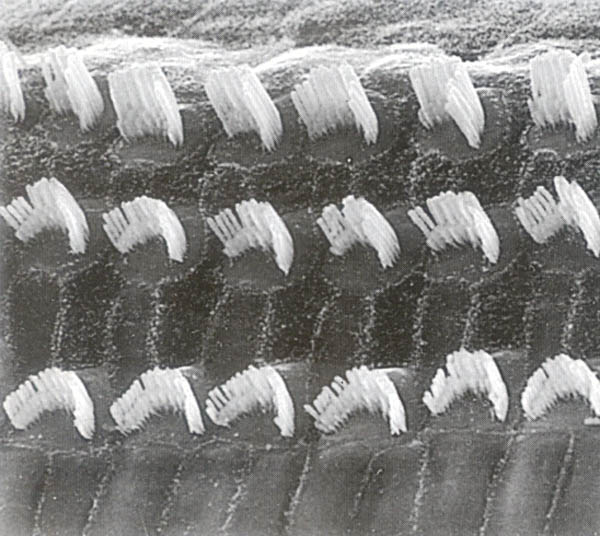
Photo N
The following is a simplified version of how we hear, as the full vocabulary and structural and functional details would fill yet another anatomy lesson. Sound waves travelling through the air are gathered by the pinna and EAM; they strike the drum-like surface of the tympanic membrane pushing it inward with a thrust equal to the intensity of the sound. Ergo, loud noises push the eardrum inward more than soft sounds. The tympanic membrane vibrations are transferred through malleus, incus and stapes. With each vibration the stapes pushes inward at the oval window creating corresponding shockwaves through perilymph and endolymph of the cochlear duct (Photo O – black arrows). Movements of the fluids rub the bristles of the hair cells against the gelatinous membrane creating an excitation which is transfer to nerve cells forming the cochlear nerve (Photo O). The cochlear nerve joins with the vestibular nerve (see below) to form Cranial Nerve VIII (vestibulocochlear nerve). Impulses of each Cranial Nerve VIII follow auditory pathways into the brain. Hair cells near the base of the cochlea detect high-pitched sounds, such as ringing of a cell phone; those closer to the apex detect lower-pitched sounds, such as barking of a large dog.
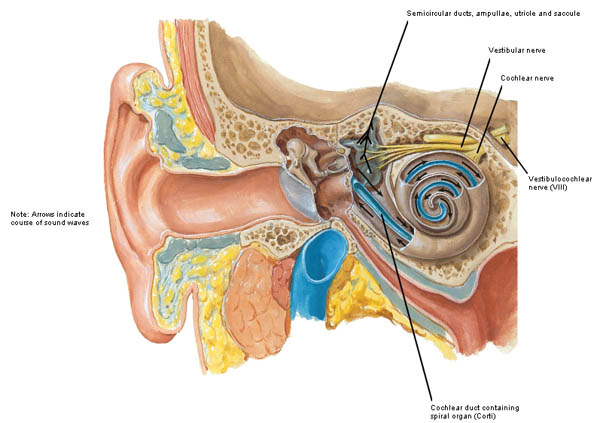
Photo O
Electrical signals carried by the cochlear nerve make their way to the primary auditory cortex of the brain (Photo P – pink zone) where electrical signals are converted into “sounds” that we learn to recognize and understand.
In summary, outer, middle and inner ears work together to transfer sound waves through air (outer ear), solid (middle ear) and liquid (inner ear) where the good, good, good, good vibrations are converted into electrical signals that make their way to the brain for interpretation of sound. Go Beach boys!

Photo P
Do you recall this lesson began with “If a tree falls in a forest and no one is around to hear it, does it make a sound?” Take a moment to think of the answer and then read on.
The answer to this philosophical riddle is that if a tree falls in the forest it creates sound waves but a receptor must be present to convert those sound waves into sound. If any creature is present with an organ than can perceive and interpret sound waves, then the falling tree does make a sound otherwise it only makes sound waves. Make sense? Good!
Now, every anatomy lesson must tie into all things Outlander and hearing is no exception. So next is a jolly good quote from Outlander book when Claire tells Jamie she is from a waaay different time zone (Starz episode 111, The Devil’s Mark). Well, Jamie knew there was something unique about this braw and bonny lassie!
“Do you know when I was born?” I asked, looking up. I knew my hair was wild and my eyes staring, and I didn’t care. “On the twentieth of October, in the Year of Our Lord nineteen hundred and eighteen. Do you hear me?” I demanded, for he was blinking at me unmoving, as though paying no attention to a word I said.

“I said nineteen eighteen! Nearly two hundred years from now! Do you hear?” I was shouting now, and he nodded slowly. “I hear,” he said softly.
Hmmm, Jamie is thinking: I ken now why the Sassynach didna take to my leather belt spankin’! It also ‘splains her twitchy-witchy “know how.”

Now we must move on to how the inner ear provides balance and equilibrium. Our ability to balance is independent of outer ear, middle ear and cochlear parts of the inner ear but it is dependent on function of the three semicircular ducts (Photo Q – bone removed). The semicircular ducts contain endolymph and each bears an ampulla, a swelling at one end (Photo Q – red arrows). Each ampulla contains a patch of “hair cells” similar to those of the organ of Corti. Once again, the bristles are covered with a gelatinous membrane.
Anterior and posterior semicircular ducts are oriented vertically at right angles to each other. The lateral semicircular duct is slightly off the horizontal plane. Orientation of the ducts cause each duct to be stimulated by angular rotation of the head in a given plane.
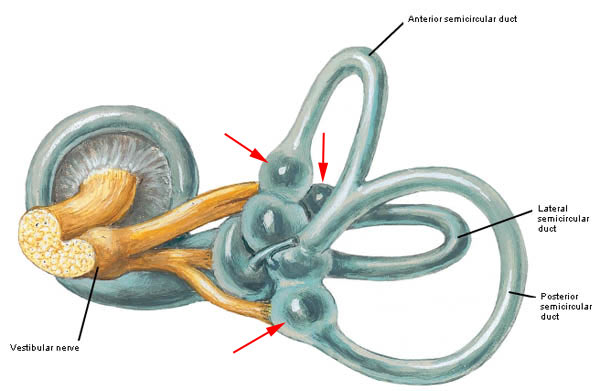
Photo Q
Turning your head from left to right sides (as in no) moves endolymph in the lateral semicircular duct. Nodding your head (as in yes) moves endolymph in the anterior semicircular duct. Moving your head to touch one shoulder or as in doing a cartwheel moves endolymph in the posterior semicircular duct. In aviation terms, the semicircular ducts are oriented such that they detect pitch, roll and yaw.
Here is how the semicircular ducts work: As the head moves in angular rotation, endolymph moves in the opposite direction bending the gelatinous membrane (cupula) and exciting the hair cells (Photo R). The hair cells transfer the signal to nerve cells of the vestibular nerve (part of Cranial Nerve VIII). The signal is carried to the brain which interprets it as angular motion of the head. The information can be used to activate various muscles to adjust the head and/or body positions.
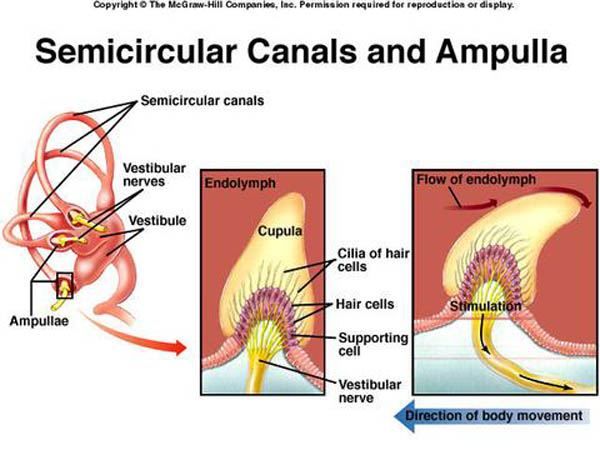
Photo R
The final anatomical elements of the inner ear are utricle (Latin meaning leather bag) and saccule (Latin meaning money bag – Dougal is into this one!) located between the semicircular duct and cochlear duct. These elements are also filled with endolymph (Photo S) and are designed to detect changes in linear acceleration or linear deceleration.
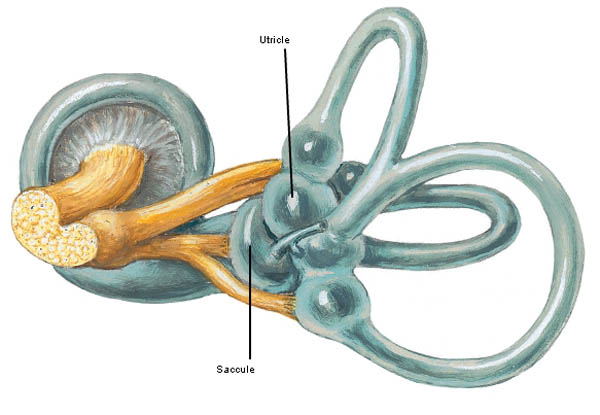
Photo S
Utricle and saccule each contain a patch of hair cells with surface bristles (Photo T – bullfrog hair cell) covered by a gelatinous membrane (absent in Photo T). The hair cells of the utricle are oriented horizontally and those of the saccule are vertically oriented.

Photo T
Seated atop the gelatinous membrane are wee otoliths (ear stones or ear rocks) made of calcium carbonate (Photo U); these add weight to the gelatinous membrane thus enhancing our sense of gravitational pull.
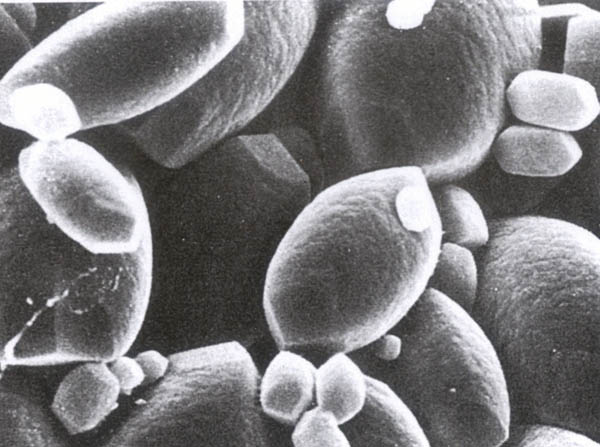
Photo U
The utricle and saccule work this way: As our head undergoes linear acceleration or linear deceleration (forward, backward, upward, downward), endolymph, the gelatinous membrane and otoconia move in the opposite direction (Photo V). This bends bristles of the hair cells causing them to activate nerve cells of the vestibular nerve of Cranial Nerve VIII. The electrical impulses are carried to the brain. The utricle detects horizontal changes and the saccule detects vertical changes in linear movements of the head. This information arrives at the brain which then determines if and how much the head is tilted and if the body needs to be reoriented in space.
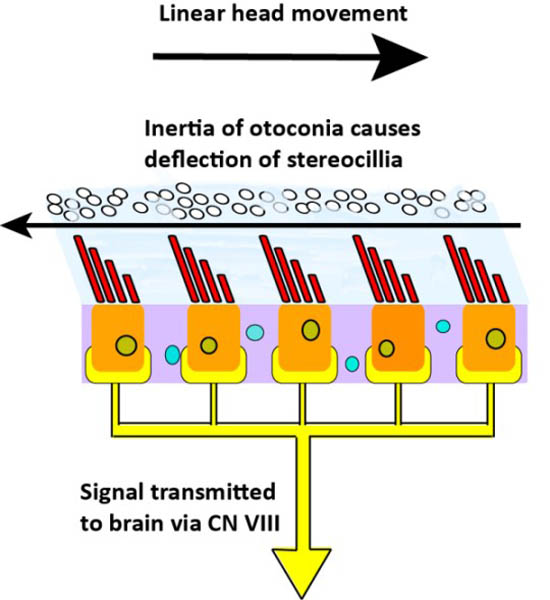
Photo V
This brings us to the end of today’s important lesson but we must tie balance and equilibrium into Outlander. Here are a couple of great quotes from Outlander book. The book quote and the Starz images (Starz, episode 108, Both Sides Now) don’t quite match because the book scenarios weren’t filmed. Nevertheless, it is fun and you will get the idea. The first scene takes place as Frank and Claire descend from Craigh na Dun after watching the Druid’s dance. Frank, the soon-to-be Oxford professor, is so absorbed in thought he doesn’t watch where he plants his feet!
“He dropped into one of his scholarly trances … The trance was broken only when he stumbled unexpectedly over an obstacle near the bottom of the hill. He flung his arms out with a startled cry as his feet went out from under him and he rolled untidily down the last few feet of the path, fetching up in a clump of cow parsley… “Are you all right?” … “I think so.” He passed a hand dazedly over his brow, smoothing back the dark hair. “What did I trip over?” “This.” I held up a sardine tin…”

Compare and contrast Frank’s stumble-tumble with Jamie’s sure footedness (Outlander book). In this scene, it is nighttime and Jamie unerringly hauls Claire through the night:
“Jamie kept a tight hold on my arm, hauling me upright when I stumbled over rocks and plants. He himself walked as though the stubbled heath were a paved road in broad daylight. He has cat blood, I reflected sourly, no doubt that was how he managed to sneak up on me in the darkness.”
Yes, Jamie has grace, balance, and equilibrium (Starz episode 104, The Gathering). Nothing will trip-flip this kilt! Hang on tight, Claire! Snort!

You may have seen this arabesque in the teaser but let’s appreciate it anyway. Jamie throws water on burning hay, a fire set by a Watch weasle! Our highlander fireman even makes tossing water a thing of beauty. Balance and equilibrium on one foot; 17th century ballet!

At last, the time has come to report the results of Lesson #24 and the Pinna Poll! Six images of pinnae from the Starz cast (episodes #103, #109, #115, #116) were shown and votes tallied. All the ear flaps are fabulous!
Not sure if you are surprised, but the winner is:…………..drum roll………………..Jamie! Congratulations Big Red! And it was an honest count, too; no stuffing of the ballot box! Jamie garnered 38% of the votes while the remaining five pinnae were in almost a dead heat with a slight edge by bad boy BJR!
Great comments were shared by many readers including these: exquisite, lovely, charming, manly, rugged, beautiful, elfin-like, fawn-like, nibble-worthy, snuggle-worthy, elegant, awesome, symmetrical, balanced, proportionate and yum! Let’s thank our six wonderful characters and all of you for playing the Pinna Poll!

That’s it for the ear. Complex and elegant! Oh, and a word to the wise: keep music turned down a notch or two. Over the years, hair cells of the organ of Corti become damaged by excessive noise. For years, the damage has been considered irreversible although a recent study shows some promise using a gene-activating drug regime. Stay tuned.
Closing with this fun poem from Mr. R’s World of Math and Science:
An ear splitting sound!
A crash and a boom!
Ringing so loudly,
It shook the whole room!
But I didn’t hear it,
I couldn’t at all,
My left and right ear,
Had gone to the mall!
My left and right ear,
My organs that hear,
Had gone to go shopping,
And that’s what I fear…
Without my 2 ears,
That spectacular pair,
I can’t hear sound waves,
Move through the air!
The deeply grateful,
Outlander Anatomist
Photo creds: Starz, Basic Histology, Junqueira & Carneiro, 11th ed., Concise Histology, Bloom & Fawcett, 2nd ed., Netter’s Atlas of Human Anatomy, 4th ed., Clinically Oriented Anatomy, 5th ed., www.aviationknowledge.wikidot.com (ampullae), www.clearwaterclinic.com (otoliths), www.fairview.org (mastoiditis), www.kids-ond.com (ossicles), www.mhhe.com (ampula hair cells), www.sciencepoems.net (Mr. R’s ear poem), www.student.com (ossicles with inner ear), www.teachmeanatomy.info (mastoid air cells), www.otopathologynetwork.org (ossicles on dime), www.wallpaper.com (fallen tree), www.wikipedia.org (mastoiditis with subperiosteal abscess)
Hallo and welcome to Anatomy Lesson #21: Smallpox. This lesson represents a departure from our usual discussions which emphasize gross anatomy. Today, we will learn about smallpox via microscopic anatomy, immunology and history! Please consider this but a brief respite from our studies of the upper limb – a topic we will return to in Anatomy Lesson #22. Outlander book readers will understand that we must make our way to the hand and very soon!
Now, how do we find ourselves learning a lesson about witches, devils and smallpox? Well, it is the machinations of that pretty little liar Laoghaire (not the actress, who is fantastic!). Yep, this 16-year-old got a witch-itch to dispose of Claire Fraser once and for all (Starz episode 111, The Devil’s Mark)! She exploited and manipulated the good and holy people of Cranesmuir to arrest, try and burn Mistress Fraser for witchcraft: she and that awful Father Bain (doesn’t he just give you the creeps?). Now, there’s a match not made in heaven!

No surprise that Geillis was accused of witchcraft being a long-time practitioner of the murky arts. And, we all kent she was something wild ever since she drank port while sporting those awesome shoon (Starz episode 103, The Way Out)! Talk about Red Shoe Diaries…for haggis sake! Takes loads of grit to don those red 18th century Christian Louboutins!

Fast forward through the trial, Claire’s skelping (ouch!) and Jamie’s bulldozer arrival: next thing Geillis pulls down her gown to reveal the devil’s mark. No more than a lowly smallpox vaccination scar (Starz episode 111, The Devil’s Mark) Geillis declares it proof that that she had lain with her master, beelzebub, and will now bear his spawn (Hum…….not a nice thing to say about Dougal!). Herself records (Outlander book):
“…It was something else I had seen that chilled me to the marrow of my bones. As Geilie had spun, white arms stretched aloft, I saw … A mark on one arm … Here, in this time, the mark of sorcery, the mark of a magus. The small, homely scar of a smallpox vaccination.”

Well, the fat is in the fire now as a gang of guys hoist Geillis off to the roasting spit! Headed for the witch’s pyre, Geillis still sports those awesome red booties: now, a girl has to look her best even if it’s for her own barbeque!

Whoa! What with all the brouhaha we shouldna forget that Claire bears her own smallpox vaccine scar! Yes, if you took the midterm practical exam (Anatomy Lesson #18) you witnessed foreshadowing: Claire’s left arm as she kisses Jamie (Starz episode 107, The Wedding). To be sure, the red arrow points to her vaccination scar proving she came from the 20th century. We book readers (not meaning to sound snooty here) already knew this scar would become an issue in future episodes. It’s good thing that neither the villagers nor Father Bain saw that scar or Claire would have been kindling!

Next, let’s study smallpox: its history, cause, signs and symptoms and the vaccination that prevents it. Hey, now wait! Please don’t haste away in fear and loathing. True, smallpox isn’t a sexy topic but it is very interesting stuff. I’ll even throw in Starz images, book quotes and historical paintings to keep you focused on the lesson. And, I’ll warn you before any gruesome pics arise (because smallpox isn’t pretty). Promise!
In Europe, smallpox was originally known as the “pox” or “red plague”. The term smallpox was first coined in 15th century Britain to distinguish smallpox (one word) from the great pox (two words). What is the great pox? Well, the great pox is syphilis, an entirely different disease, different cause, different symptoms and different treatment. Of the two diseases, however, smallpox is by far more deadly.
Sufferers of syphilis classically exhibit three stages but stage two is characterized by a non-itchy rash and hence the term “pox.” Photo A is a 16th century woodcut illustrating the rash of secondary syphilis. But, enough great pox for now; we will return to it in a future anatomy lesson.
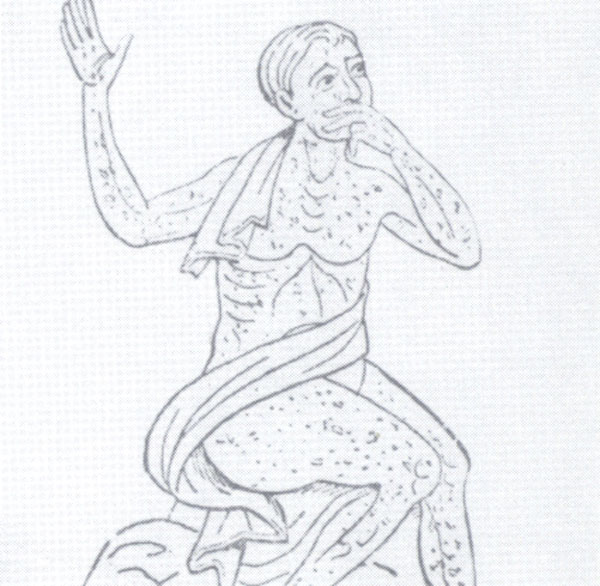
Photo A
Back to smallpox. We’ll approach this disease in an orderly manner by following its structure, history, signs and symptoms, treatment and prevention. Warning: this lesson includes three graphic images showing sufferers with full-blown smallpox. If such images bother you, an advanced warning will allow you to skip them.
Here is your warning sign:

Here is your “it’s safe to peek” sign:

Smallpox is an acute, contagious disease which derives its name from the Latin meaning “spotted” or “pimpled” referring to raised bumps or pustules that cover skin of the afflicted. Smallpox is not caused by a bacterium (sing.) but by the variola virus a large brick-shaped member of the poxvirus family (Photo B – transmission electron microscope – TEM image).
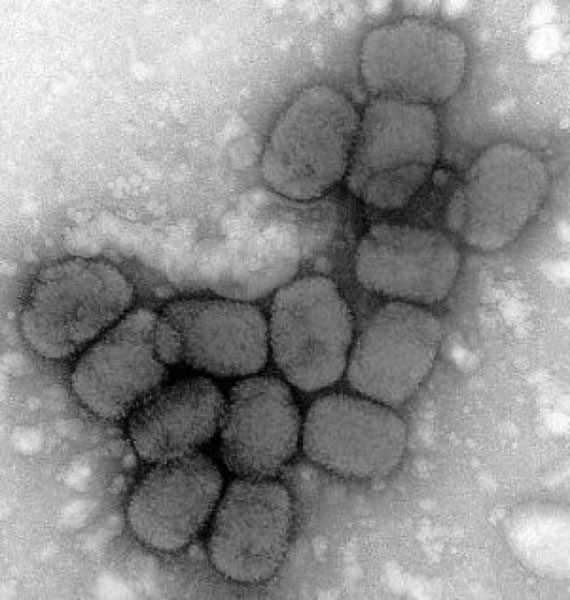
Photo B:
The following image (Photo C – TEM image) reveals the internal structure of the variola virus. Understand that the virus is essentially colorless – the image colors are computer generated. The red-orange dumbbells represent the complex viral core. Too technical? Then, let’s move to the history of smallpox.
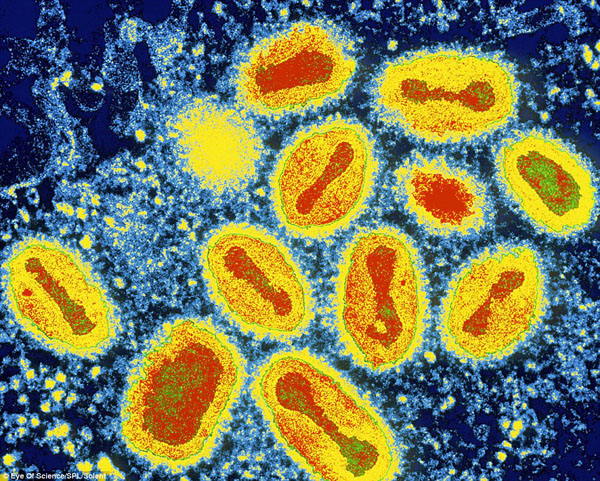
Photo C
The history of smallpox is fascinating in that it altered the course of human history and even contributed to the decline of civilizations. It is no understatement to declare that smallpox ranks among the most devastating illnesses ever suffered by mankind and probably contributed to the vintage curse “a pox on thee.” Smallpox routinely killed at least one third of its victims. Sadly, the survivors of this dreadful pestilence were often left with major disfigurement or disability. Even more devastating is that governments have been known to intentionally infect groups of people with the disease to eradicate them from a desirable area. This lesson won’t be addressing those atrocities in detail but it bears mentioning because for centuries, people have known how crippling this disease is to communities.
Smallpox is believed to have evolved from a rodent virus between 16,000-68,000 years ago; the wide time range is due to different estimates of genetic change during evolution, the so-called molecular clock. Evidence suggests that smallpox jumped to humans about 10,000 BCE. The earliest physical evidence of the disease comes from Egyptian Pharaoh Ramses V who died in 1157 BCE (Photo D). His mummified remains show the telltale skin pockmarks. Numerous old manuscripts record what appear to be waves of smallpox epidemics that repeatedly struck the Eastern hemisphere.
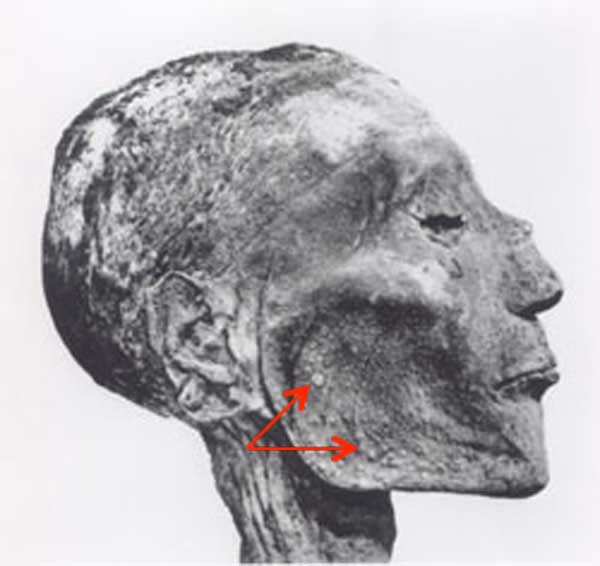
Photo D
The clearest description of smallpox from pre-modern times is credited to a 9th century (860 – 925 CE) Persian physician and scholar, Muhammad ibn Zakariya ar-Razi ( Photo E – examining a child with smallpox). Known in the West by his Latinized name, Rhazes or Rasis, he was an important figure in the history of medicine as he was the first to differentiate smallpox from measles in his text, Kitab fi al-jadari wa-al-hasbah (The Book of Smallpox and Measles).

Photo E
Smallpox reached Europe between the 5th and 7th centuries CE and over time spread along trade routes into Africa and Asia finally reaching the Americas in 1519 via Spanish conquistadors. Indigenous peoples had no immunity to the disease so more than three million Aztec as well as many Inca succumbed to smallpox (Photo F – 16th century woodcut).
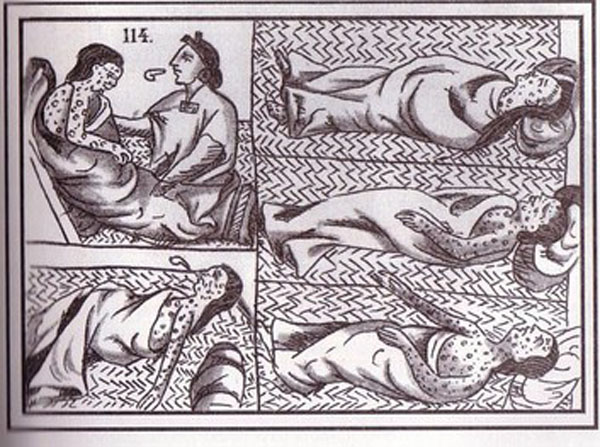
Photo F
Moving to Jamie’s time of the 18th century, smallpox is estimated to have claimed 60 million lives including five reigning monarchs and was responsible for a third of all blindness; it also marked the faces of more than half the population of Europe.
A genuine scourge, it killed 20-60% of all those infected and over 80% of infected children died from it. Jamie’s own family suffered smallpox when he was a lad. Here from Starz episode 113, The Watch and in Herself’s own words (Outlander book):
“Two red- haired, tartan- clad little boys stared solemnly out of the frame … Jamie, and his older brother Willie, who had died of the smallpox at eleven. Jamie could not have been more than two when it was painted … Jamie had told me about Willie … I remembered the small snake, carved of cherry wood that he had drawn from his sporran to show me.”

To underscore its havoc during the 20th century smallpox killed 300-500 million people globally. In 1967, the World Health Organization (WHO) estimated that 15 million people worldwide contracted smallpox with two million deaths the same year.
Smallpox is spread through direct contact with infected people or their body fluids or via fomites, contaminated objects that transmit disease (e.g. bedding). As a child at Lallybroch (Starz episode 113, The Watch – image below) Jamie had smallpox but his case was not serious. Herself explains (A Breath of Snow and Ashes book):
He considered for a moment. “I had the smallpox when I was a wean, but I think I wasna in danger of dying then; they said it was a light case.
Och! Is this possible? Could Jamie have had a light case of the smallpox? Would Herself make such an error? No problemo! Indeed, there are two main types of smallpox: Variola major, the common and most lethal form and Variola minor, a milder disease which was fatal in less than 1% of cases. We can even postulate that Jamie may have been exposed to the same variant as Willie but received a lower viral load or was less susceptible to its effects. Finally, a couple of rarer forms of smallpox invariable caused death but these lay beyond our present discussion.

The signs and symptoms of smallpox are very well known. WARNING: the next three images show full blown smallpox; please skip if you must. Watch for the kitten to know it’s safe to come out again.
After a victim inhales the smallpox virus or is infected via fomite, it has an incubation period of about 12 days during which the infected person is not contagious. During this time, the virus is busy infecting cells of mouth, throat and respiratory tract after which it distributes to lymph nodes and other structures. Like many viruses, it produces a 2-4 day prodrome (early symptoms) of mild fever, muscle pain, malaise, headache and prostration. By 12-15 days, large numbers of virus flood the bloodstream (viremia) and the first visible lesions appear on the mucosa (Anatomy Lesson #14) of mouth, tongue, palate and throat. By days 15-17 skin eruptions occur. Although smallpox is routinely categorized as a skin disease (Photo G – 1912 archival photo) understand that it also invades most mucous membranes of the body including exposed surfaces of the eye.
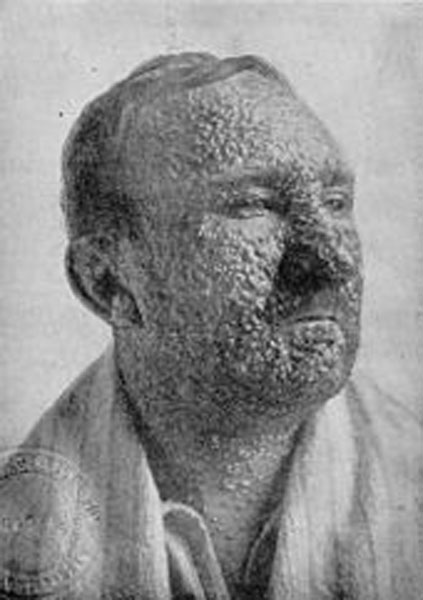
Photo G
Skin eruptions rapidly develop into fluid-filled pustules: sharply raised, round, tense and firm to the touch. The pustules traverse epidermis and dermis and are umbilicated meaning they demonstrate a central pit (Photo H – 20th century). By the end of week two the pustules deflate, dry up and form crusts or scabs. By days 16–20, scabs flake off leaving depigmented (no skin pigment) white scars.

Photo H
Another defining characteristic of smallpox lesions is their distribution: pustules cover the entire body with concentrations on the head and upper and lower extremities including palms and soles (Photo I – 1886 archival photo).
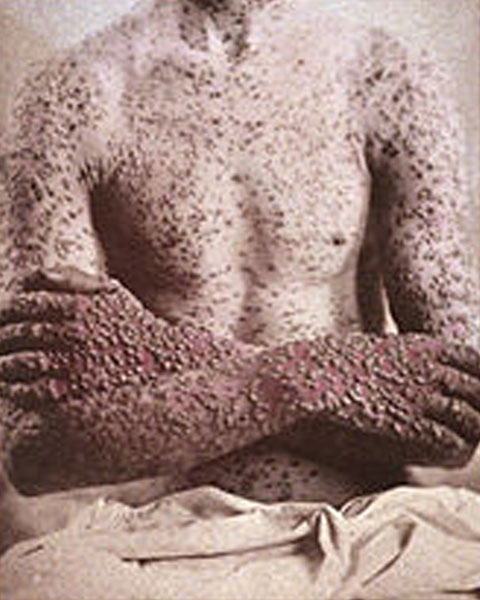
Photo I
IT’S SAFE TO PEEK NOW!
Skin distribution helps practitioners distinguish smallpox from chickenpox lesions which are concentrated on the trunk and less numerous on the extremities (Photo J). In addition, all smallpox skin lesions are of the same maturity (see Photo I) whereas chickenpox lesions present in various stages of maturity: old healing lesions intermix with new developing lesions.
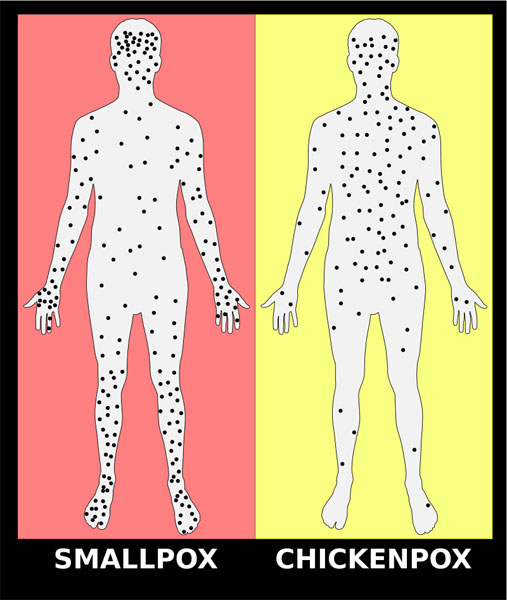
Photo J
Next, let’s consider how smallpox leaves scars or pockmarks as a “gift that keeps on giving.” If you read Anatomy Lesson #5 and Anatomy Lesson #6, you learned the structure of skin and its appendages. As a quick review, skin is divided into an outer epidermis and a deeper dermis (Photo K) which in turn is bound to subcutaneous tissue (not part of skin). Skin bears a number of appendages including hairs, arrector pili muscles, sweat glands and sebaceous glands. Sebaceous glands produce sebum, a waxy-oily substance that is secreted into hair follicles or via small ducts leading to skin surfaces. Sebaceous glands are found in all skin except that of soles and palms and they are most numerous on the face. The awful smallpox lesions extended deeply into the dermis where they destroyed sebaceous glands. In the aftermath of healing, deep white scars (pockmarks) were left everywhere on the skin but were densest and most disturbing on the face, the body part by which the world identifies us.
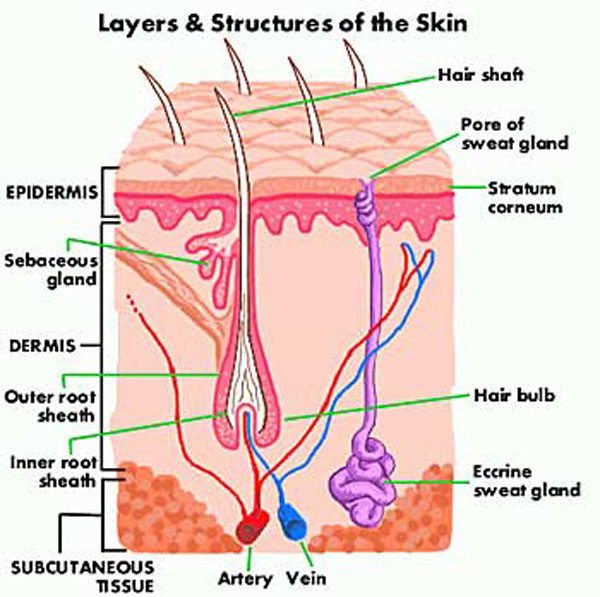
Photo K
If an individual survived smallpox, long-term complications included pockmarks, blindness, arthritis, osteomyelitis (bone marrow infection), pneumonia and encephalitis. On the plus side and there was only one plus, sufferers typically developed immunity to subsequent smallpox outbreaks.
Many famous historical people suffered the ravages of smallpox. These include Queen Elizabeth I who in 1562 was so scarred by smallpox that she was left half bald and dependent upon wigs and heavy lead-based makeup to cover her pockmarks (Photo L – Armada portrait by George Gower). During this era, ideal beauty and wealth was marked by very pale, white skin. To achieve this look, people applied a foundation of lead and vinegar, even using mercury in makeup, which presented it’s own health problems.

Photo L
Truly a global scourge, the following is an incomplete list of famous historical figures that either died of or were disfigured by smallpox:

Photo M
Hey, am I losing you? Well, here, this will jolt ye awake! I said this wasna going to be a sexy lesson, but the next image shows that I, um, clearly lied. Only Jamie could turn buttering and eating a piece of bread into global cardiac arrest. Grab the paddles! Stand clear!

Now let’s turn to treatment and prevention of smallpox. First the bad news and then the good: The bad news is treatment for smallpox is minimal. A smallpox vaccination given within three days of exposure can lessen the disease but otherwise supportive therapy such as fluid administration is the order of the day. The good news is smallpox can be prevented. A brief history of its prevention follows.
The earliest procedure to prevent smallpox was variolation wherein powered smallpox scabs (ugh!) were inhaled through the nose (oh!) or pus from smallpox lesions (yuck!) was scratched into the skin. Although disputed by some, this may have been practiced in India as early as 1,000 BCE. Undisputed are accounts of variolation performed in China by the 10th century and widely practiced by the 16th. If successful, variolation produced lasting immunity to smallpox. However, it was an iffy practice because a variolated person could get full-blown smallpox from the procedure and transmit it to others. Why then was it practiced? Because variolation caused 2% mortality rate compared to 30% + mortality rate for smallpox!
The next procedure to prevent smallpox is credited to Edward Jenner (1749-1823), an English country doctor of Gloucestershire. Jenner (Photo N) was a private student and lifelong friend of the great Scottish surgeon, anatomist and naturalist John Hunter (Anatomy Lesson #3).

Photo N
As a country doctor, Jenner heard dairymaids with cowpox pustules on their hands (Photo O) claim that they could not get smallpox: “I cannot take the smallpox, since I have had the cowpox.” Medical men of the day were aware of these claims but most dismissed them as folk lore. Jenner, on the other hand, was so intrigued he made observations and studied cowpox for over a quarter of a century. From John Hunter, he received the following famous bit of advice: “Why think? Why not try the experiment?”
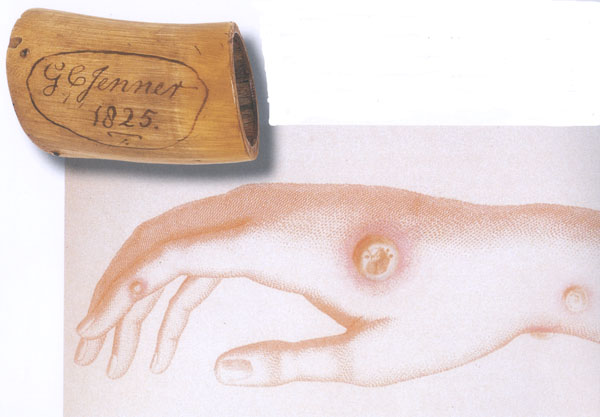
Photo O
Finally in May of 1796, Jenner did the experiment: he removed “matter taken from the sore on the hand of a dairymaid” (Photo O – Sarah Nelmes) and inserted it into skin scratches on the arm of eight-year-old James Phipps, son of Jenner’s poor landless gardener (Photo P).
Are you horrified? But of course you are! In today’s western world of informed consent and scrutinized research protocols such a thing would be absolutely prohibited: different times, different rules.
Back to the story: seven days after the procedure, James experienced chills, loss of appetite and slight headache but the next day felt fine. Then on several occasions in 1796 Jenner did the unthinkable: he inoculated James with smallpox matter and the boy experienced no disease whatsoever! Jenner presented his findings to the Royal Academy, but more importantly, he had the foresight to publish them in a 1798 booklet explaining how inoculation with cowpox caused immunity to both cowpox and smallpox and thus was born the procedure later termed vaccination.
How did the vaccination work? Well, cowpox is caused by cowpox virus a poxvirus which is molecularly similar to the smallpox variola virus so the body’s immune system creates protective and memory cells that upon subsequent exposure will attack and destroy the smallpox virus.
In fairness, Jenner was not the first to inoculate people with cowpox virus to achieve smallpox immunity: others included Benjamin Jesty (farmer- Dorset, England) who performed the procedure on family members in 1774 and in 1791, Peter Plett from the Duchy of Holstein (now Germany) inoculated three children. The reason Jenner is credited with the feat is because he was the first to publish his findings as advised by the sage academic adage: publish or perish! His publication even included the drawing of Sarah Nelmes’ hand and a cupping horn in which he transported cowpox-infected matter for vaccination (Photo O).

Photo P
A wee bit more history and then we move on: In 1809, the first U.S. state began compulsory public vaccination against smallpox. England introduced compulsory infant vaccination via the 1853 Vaccination Act. Other European countries established similar programs but many were fraught with problems and rebellions by the general public.
The last and current smallpox prevention method involved switching from cowpox virus to a related virus for vaccination: Also known as vaccinia virus, this poxvirus is molecularly similar to both smallpox and cowpox and some think it may be a hybrid of the two; the precise origin of the modern vaccinia virus has become lost.
WARNING: If needles make ye queasy, ye may want to look for that kitten agin.
Here is how current day vaccinia vaccination is performed: The vaccine is not given with a hypodermic needle and thus is not a “shot” like many vaccinations. Rather, the vaccine is given using a bifurcated (two-pronged) needle (Photo Q).
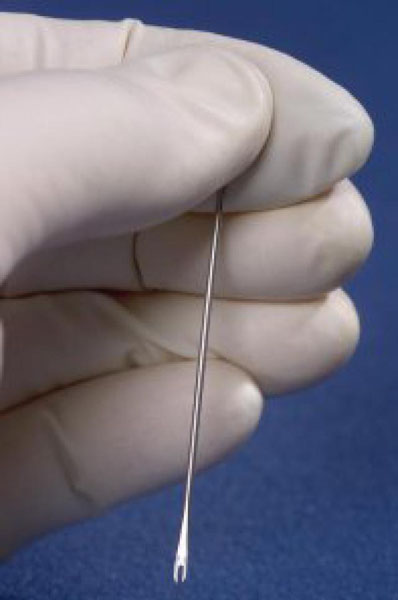
Photo Q
The needle tip is dipped into vaccine solution such that the prongs retain a droplet of fluid (Photo R).

Photo R
The upper arm is then quickly pricked several times with the needle (Photo S). The pricking is not deep. Did you notice I use the present tense? Yes, the vaccine is still given even today but not to the general public.

Photo S
If vaccination is successful, 3-4 days later, red and itchy bumps develop at the vaccination site where the body’s protective cells (lymphocytes) react to foreign molecules of the vaccinia virus (Photo T). After a week, the bump becomes a large pus-filled blister. At week two, the blister dries up and forms a scab. The scab falls off during the third week, leaving a visible scar. The size of the scar depends on the intensity of an individual’s reaction to the vaccine.
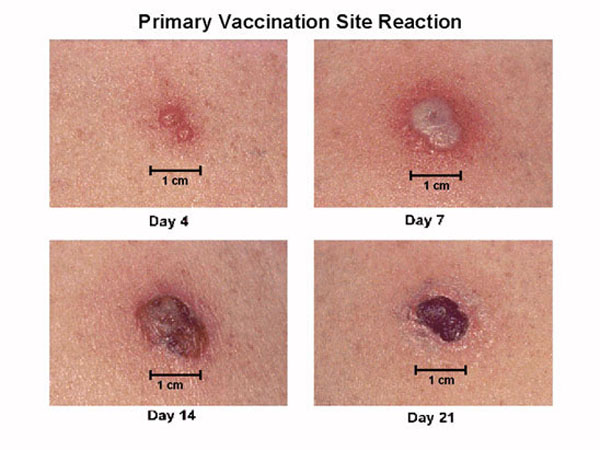
Photo T
OK! IT’S SAFE TO PEEK NOW!
Back to smallpox history, after vigorous public vaccination campaigns throughout the 19th and 20th centuries, the last recorded case of naturally-occurring smallpox was in Somalia in 1977. Three years later, WHO declared that smallpox was eradicated from the world, a feat that is generally regarded as one of the greatest triumphs of modern medicine. So officially the deadly virus no longer exists in nature!
Personally, I cringe when humans make sweeping statements about nature as they evoke the follies of human hubris. Claire reflects on such an issue in The Fiery Cross (book 5 of Outlander series):
“This was in fact likely. However, I was quite aware of the old adage— “Man proposes and God disposes” … ” (From the Latin text by Thomas à Kempis: For man proposes, but God disposes; neither is the way of man in his own hands.”)
OR
In the more colorful words from Scottish poet Robert Burns in his 1785 poem “Tae a Moose, on Turning Her Up in Her Nest with the Plough: The best-laid schemes o’ mice an’ men Gang aft agley.”!
OR
In the words of Professor Ian Malcolm from the film, Jurassic Park: “Life finds a way.”
Will smallpox stay buried for good? We certainly hope so!
Let us end this lesson with more fun and games: we return to our hero and heroine in Starz episode 111, The Devil’s Mark. I love the trial wherein Jamie and Claire together witness Geillis’ confession. Take a gander at Claire’s glass face!

Oh, my! Jamie watches as Geillis exposes her “mark of the devil” and Claire suddenly kens that Geillis is a 1968 time traveler and her “devil’s mark” is naught but a lowly smallpox vaccination scar!

But, here is the moment of truth! Jamie’s nimble brain is churning fiercely as he realizes that Geillis has given him the chance to hie Claire out of that bloody inquisition. RUN! Wow. Jamie’s eyes could act all their own only that would be gross so…never mind…but ye ken what I mean! So expressive!

After getting Claire away from Cranesmuir and into a quiet wooded area, Herself records Jamie’s reaction (Outlander book):
“I said before that I’d not ask ye things ye had no wish to tell me. And I’d not ask ye now; but I must know, for your safety as well as mine.” He paused, hesitating. “Claire, if you’ve never been honest wi’ me, be so now, for I must know the truth. Claire, are ye a witch?” I gaped at him. “A witch? You— you can really ask that?” … “Yes, I am a witch! To you, I must be. I’ve never had smallpox, but I can walk through a room full of dying men and never catch it. I can nurse the sick and breathe their air and touch their bodies, and the sickness can’t touch me. I can’t catch cholera, either, or lockjaw, or the morbid sore throat. And you must think it’s an enchantment, because you’ve never heard of vaccine, and there’s no other way you can explain it.”
With her vaccination scar clearly on display, Claire tearfully explains her own “devil’s mark” to Jamie.

Jamie (this man is a true wonder) does believe her and her heart; he kens she is telling him the truth and pledges that he will believe whatever she tells him. So, she tells him everything from the get-go including stone travel, combat nursing and boring Frank! Yikes! And all’s well that ends well for oh, say, two hours. Nice job to the entire cast and crew for that mind-numbing, stomach-rolling, breath-holding, teeth-grinding rollercoaster ride!

However, honesty compels me to declare the true devil’s mark from Starz episode 111. Who is nominated for this honor? Drum roll!!!! And, the winner is: the puir, misunderstood little gal Laoghaire. Who is this bonny lass with more facets than a well-cut stone? Watch her face change as she hisses at Claire!
A daughter accused by her own father of loose behavior?

The innocent “virginal” seductress of love-of-her-life Jamie?

The darling, needle-wielding granddaughter of Mrs. Fitz?

The cunning author of Claire’s imprisonment and verdict?

Or, a tiny dancer who will gladly execute (so-to-speak) a pirouette atop Claire’s ashes?

Hope ye all ken by now that if Starz episode 111 has a devil’s mark it surely is this calculating, cunning and cruel Bad-Lass!
Ending on this somber note of justice gone awry, I do hope you all learned something new today: “Let’s rise and be thankful, for if we didn’t learn a lot today, at least we may have learned a little…” (Born for Love: Reflections on Loving, Leo Buscaglia).
A deeply grateful,
Outlander Anatomist
Image creds: “Great Moments in Medicine”, 1961 paintings by Robert A. Thom, “Medicine: Perspectives in History and art, www.bioteach.unl.edu, www.crateandbarrel.com, www.dailymail.co.uk, www.dermatologyabout.com, www.healthline.com, www.mayclinic.org, www.ncbi.nim.nih.gove, www.who.int, www.wikimedia.com, www.wikipedia.com, www.onlinelibrary.wiley.com, www.2.lbl.gov, www.socialphy.com, www.momentummoonlight.com.