
Greetings all Anatomy Students!
What do I mean by Sam’s surface? I refer to his surface anatomy, also know as topographical anatomy. This branch of anatomy identifies structures from features expressed at the body surface. It does require anatomical knowledge by the user and is non-invasive.
Over the years, I have received many images of Sam and Jamie from followers asking me to apply arrows and identify structures. This lesson is a compilation of some of these images. I hope you enjoy as much as I do. 😉
So, let’s get started!
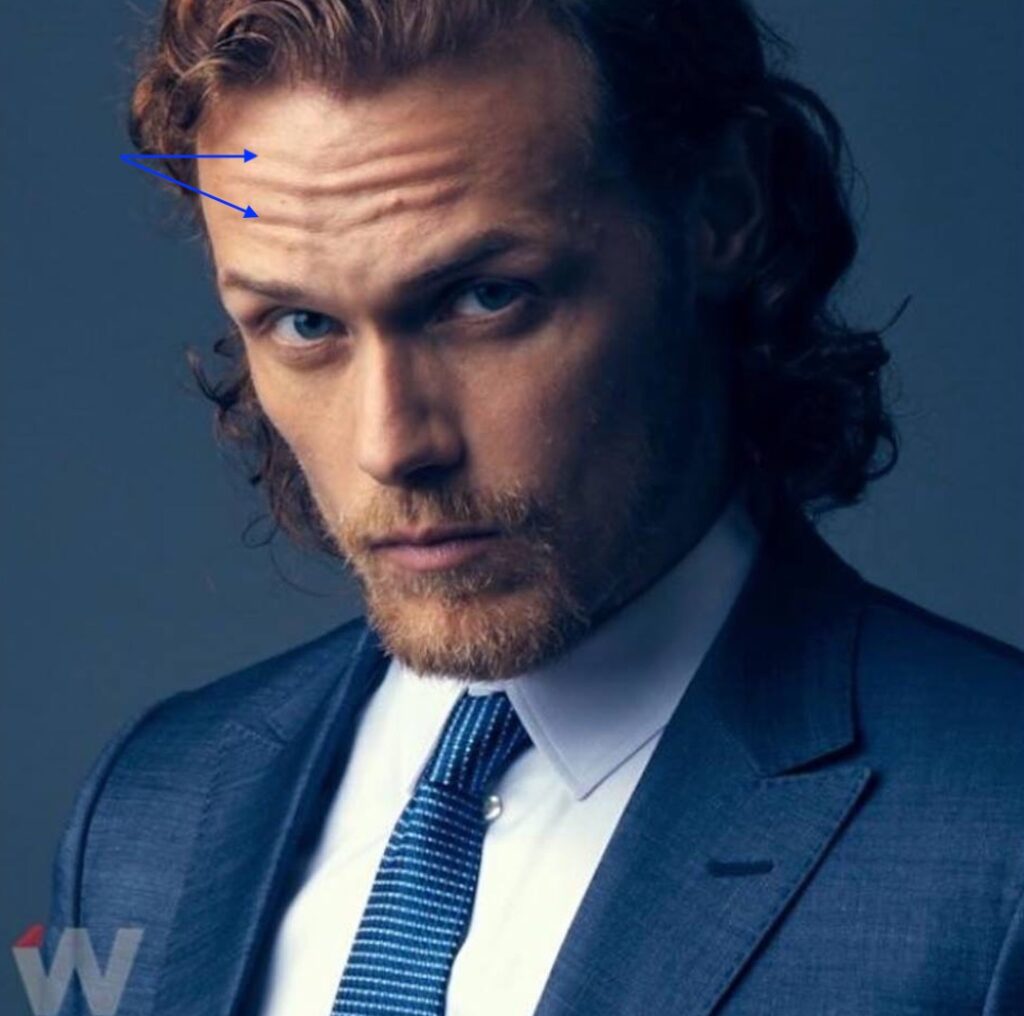
Frontalis: Paired muscles of facial expression, frontalis fibers run vertically in the forehead. When they contract, they lift the brows and produce horizontal wrinkles of forehead skin, conveying concentration and concern. Perfect example from model Sam (blue arrows).
Corrugator Supercilii: Paired muscles of facial expression from the nose side to the middle of each eyebrow. Upon contraction, corrugators draw the brows together and down producing small vertical wrinkles between the brows and a small bulge of skin above the brows. Jamie and Murtagh show corrugator prowess (red arrows) as they watch the King of France during his a “private” moment (Outlander, episode 202 “Not in Scotland Anymore!” 😱

And, this image from outlander episode 708 “Turning Points,” shows an outstanding example of corrugator supercilii (red arrows) as Jamie realizes he almost shot his son during the second Battle of Saratoga! 🥺

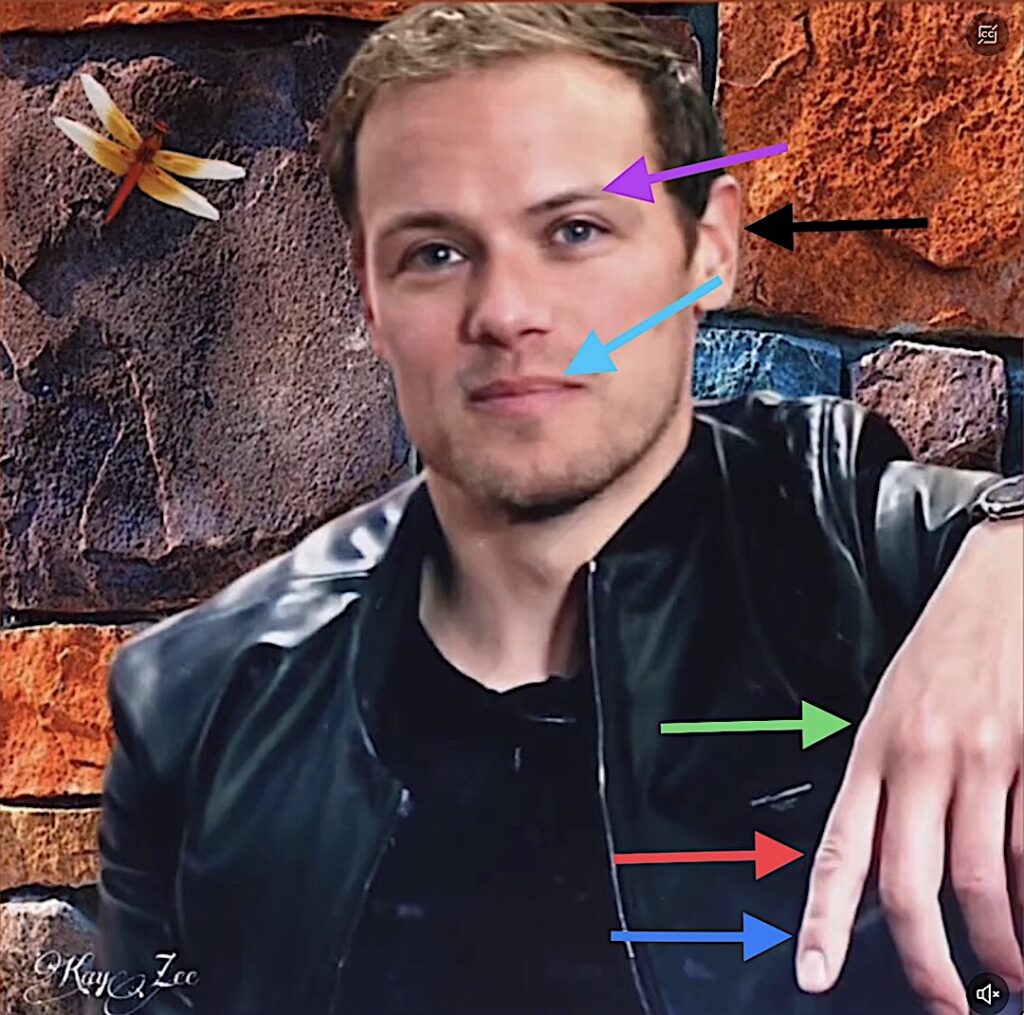
Procerus: Procerus are muscles of facial expression wrinkling the skin over the bridge of the nose and flaring the nostrils. Results? They help create an expression of anger. “Who are you calling a procerus?” threatens Sam (red arrows). 😆

Supercilium: As everyone kens, eyebrows add to facial expression. Anatomically, the eyebrow is the supercilium (super silly, huh?). Sam has naturally thin, beautiful brows (purple arrow). I recall him being asked at during an interview if he plucked them, to which he responded, “Never.”
Vermilion Border: The vermillion border is intersection between facial skin and the rim of lips (turquoise arrow). Sam’s border forms a lovely Cupid’s Bow in the midline.
Moving on to the hands….
Metacarpophalangeal Joint: This joint (green arrow) is formed where the metacarpals of the palm meet the proximal phalange, the first and largest finger bone.
Proximal Interphalangeal Joint: This is the intersection between proximal phalange and middle phalange (red arrow).
Distal Interphalangeal Joint: This joint occurs between middle phalange and distal phalange (blue arrow).
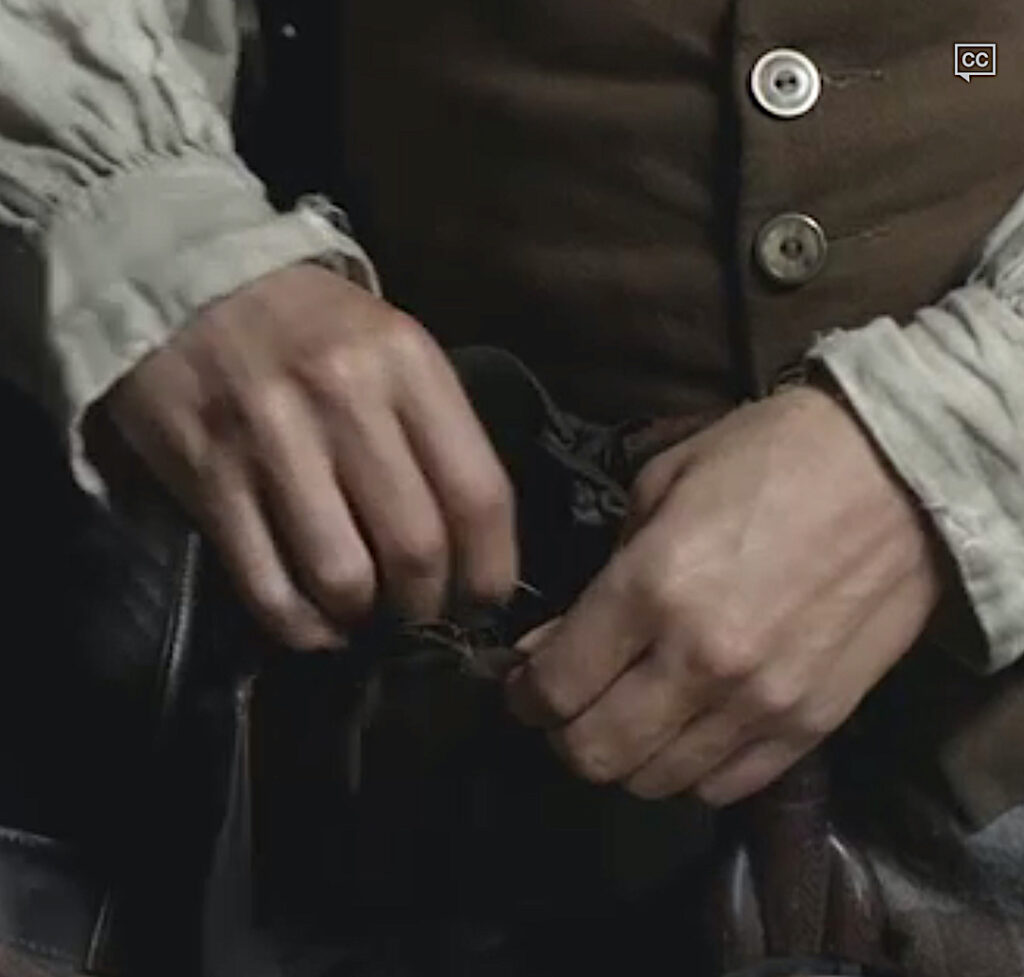
Attention: The wonderful image below is the property of @KayZee. ❤️
Didn’t everyone notice Sam’s beautiful hands as he discusses Claire with Murtagh before the wedding in Outlander Episode 107, “The Wedding.” 😍
Moving on to the torso…
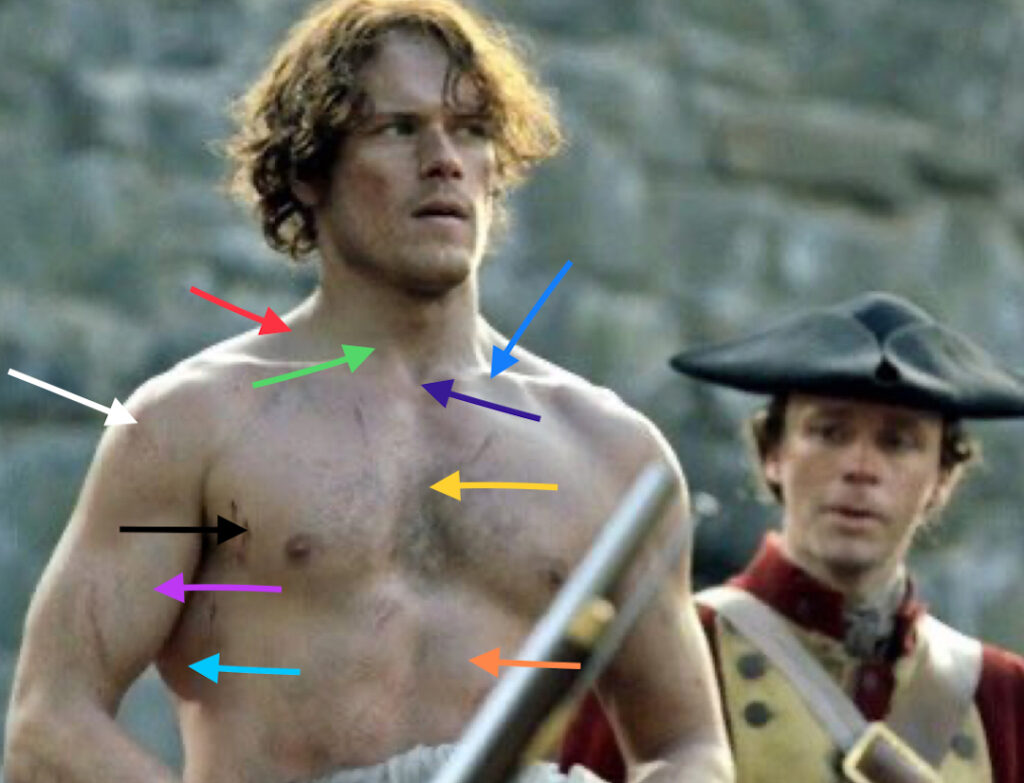
The next image is JAMMF between floggings – Outlander episode 106, “The Garrison Commander!” 😱 Lots of arrows on this one and the list is loooong but so worth it!
Trapezius: Trapezius (red arrow) is a massive flat triangular-shaped muscle that is paired. Together, they lift the shoulder joint and pull the shoulder joint back and down.
Clavicle: Commonly known as the collar bone (turquoise arrow), the paired clavicles are 6″ S-shaped bones between sternum and each shoulder joint. Clavicle is also the most commonly fractured bone of the body (one of my grandsons fractured his last year). It holds the shoulder joint away from the sternum allowing for greater mobility of the arm.
Fun Fact: Dogs and cats don’t have clavicles so their shoulder blades shift to lie at sides of the torso; ours lie over our backs. Thus, their front limbs move forward and back whereas, ours can rotate almost 360°. The human shoulder joint is the most movable joint of the human body, all because of the clavicle! 🤩
Sternocleidomastoid: Paired strap-like muscles (green arrow) joining sternum (breast bone) and clavicle to skull behind ear. Acting alone, each muscle flexes the neck toward the shoulder and rotates the chin toward the shoulder. Together, the muscles draw the chin toward the sternum.
Fun Fact: Sternocleidomastoid muscles are one of over 20 pair of muscles acting on the neck! 🤓
Suprasternal Notch: This bony landmark (purple arrow) indicates the top of the sternum. Intrathoracic pressure can be measured via the soft tissues above this landmark.
Sternum: The sternum (yellow arrow) is an unpaired bone which forms the front of the chest. It provides attachments for clavicles and first seven pair of ribs. It also supports and protects vital organs such as heart and lungs.
Rectus abdominis: This paired muscle (orange arrow) forms the belly on either side of the midline. Each muscle is long and flat, extending from sternum and ribs to pubic bone. Acting together, they bend head toward pelvis.
Deltoid: The deltoid (white arrow) is shaped like an inverted triangle and overlies the shoulder joint, giving the shoulder its rounded contour. It helps raise the arm forward, to the side and backward. It is subdivided into anterior (front), middle, and posterior (back) sections.
Pectoralis Major: The term pectoralis is derived from the Latin meaning “breast.” Gyms refer to them as ‘pecs.” Pec major is paired and the largest muscle (black arrow) of the chest They draw the clavicle downward. They also raise the arm forward, pull arm against torso, or rotate arm toward sternum.
Biceps Brachii: The biceps (pink arrow) are the large muscles at the front of the arm. They create the fabulous bulge that Popeye made famous. In Latin, biceps means “two heads,” so named because the muscle originates from two different parts of the scapula. Biceps flexes the elbow joint and rotates the palm forward/upward. It also flexes the shoulder joint and draws the humerus (arm bone) against the torso.
Fun Fact: Contrary to popular opinion, biceps is not the prime mover of the elbow joint! A deeper lying muscle, brachialis, is the prime mover. 💪🏻
Latissimus Dorsi: Latissimus dorsi (aqua arrow) is a large flat muscle of the back. It inserts on the humerus pulling it backwards, against the body, and towards the sternum. Sam’s latissimus is massive! 🥳
 and
and
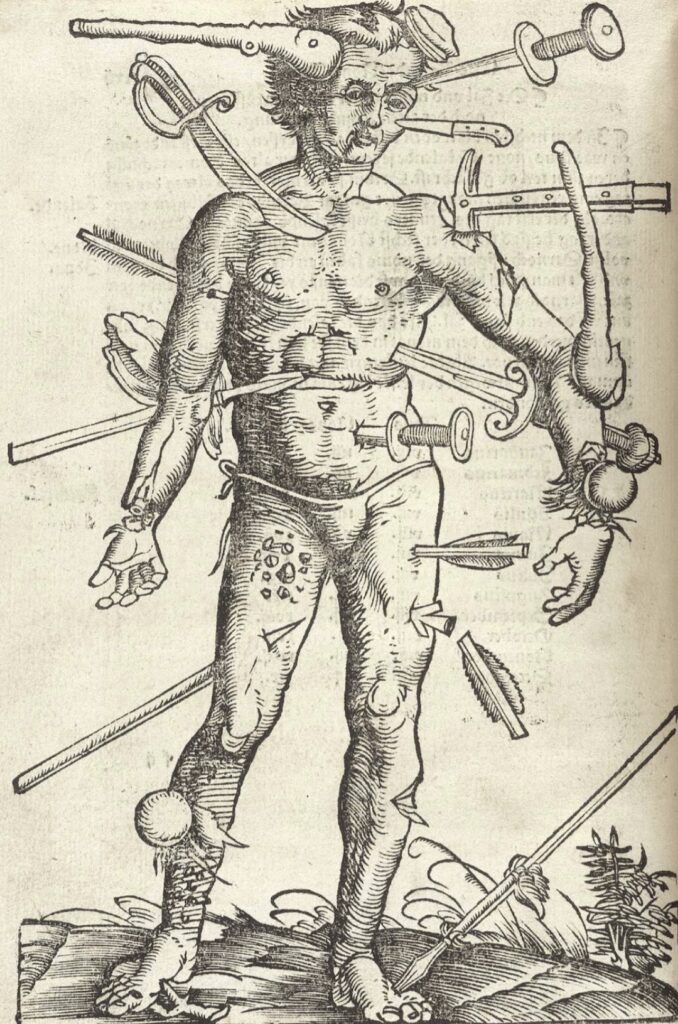
The previous image of Sam as Jamie reminds me of “The Wound Man,” a surgical diagram that appeared in European medical texts of the fourteenth and fifteenth centuries, up until the 1700s. It showed various battle injuries and diseases that a medical practitioner might encounter. Cures were listed on nearby pages. A horrifying image, for sure! 😳
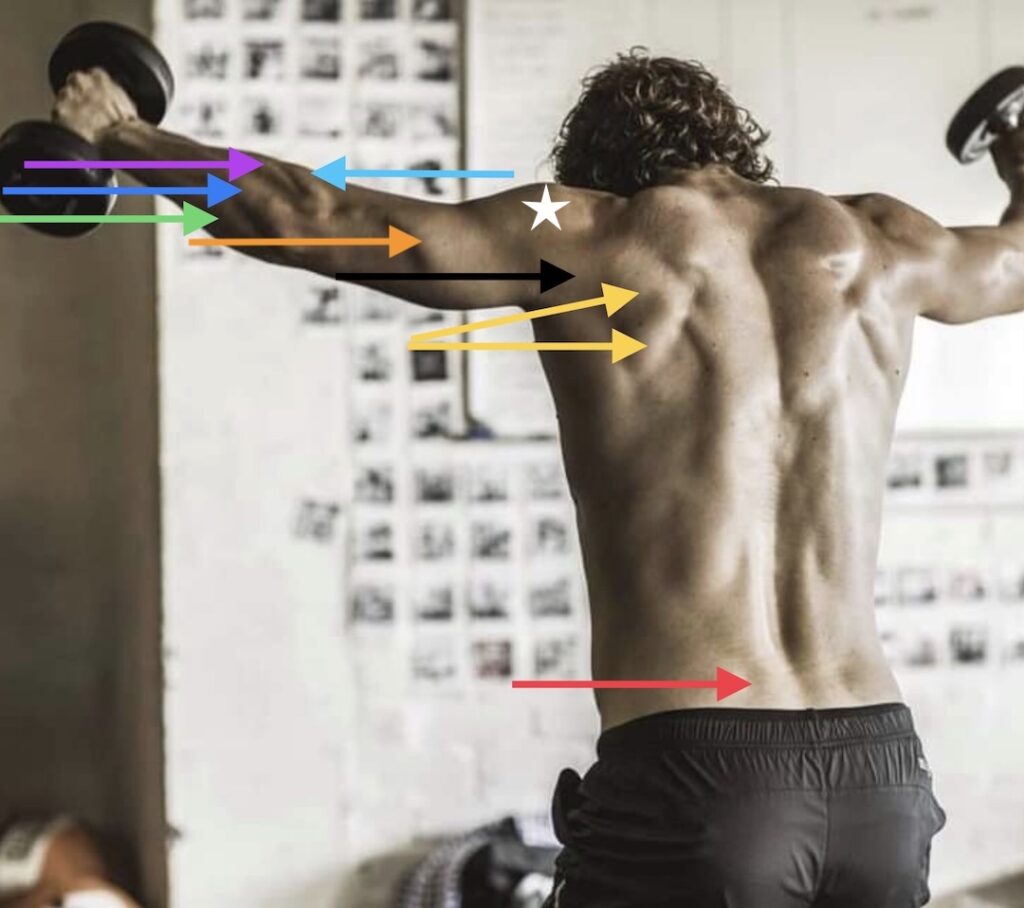
Next, Sam’s back is a marvelous roadmap of topographical anatomy.
Infraspinatus: This muscle (yellow arrows) extends from scapula (shoulder blade) to humerus (arm bone). It externally rotates and stabilizes the shoulder joint. Along with three other muscles, it helps form the rotator cuff of the shoulder joint.
Triceps Brachii: The triceps (orange arrow) derives its name from Latin meaning three heads because it takes origin from the scapula and two different areas of the humerus. It ends on a forearm bone, the ulna. It extends (straightens) the elbow joint.
Brachioradialis: This muscle (aqua arrow) attaches humerus to radius, a forearm bone. It helps flex the elbow joint.
Extensor Carpi Radialis Longus: This forearm muscle (violet arrow) reaches from humerus to second metacarpal bone. It extends (straightens) wrist and abducts hand (moves hand toward thumb).
Extensor Digitorum: Extensor digitorum lies next to extensor carpi radialis longus (blue arrow). It extends all four fingers (not thumb). Straighten your bent fingers. Extensor digitorum did that!
Extensor Carpi Ulnaris: This forearm muscle (green arrow) reaches from humerus to fifth metacarpal bone. It extends the wrist and adducts the hand (moves hand away from thumb).
Posterior Deltoid: The deltoid was explained above but now we add a caveat. Sam’s posterior deltoid (black arrow) is unusual because a distinct groove separates it from middle deltoid (white star). Most people do not exhibit this distinct separation.
Erector Spinae: This massive muscle (red arrow) is paired; it has several parts based on origin and insertion of the muscle fibers. Working together, erector spinae straightens the back; working alone, it rotates the back.
Next is Sam in a full plank position with elevated feet. This one has a number of repeated structures, but is still delightful to view. 🤩
Trapezius: Yellow arrow – see above
Deltoid: Blue arrow – see above
Pectoralis Major: Pink arrow – see above
Biceps Brachii: Violet arrow – see above
Latissimus Dorsi: Aqua arrow – see above
Rectus Abdominis: Orange arrow – see above
External Abdominal Oblique: The EAO is the largest flat abdominal muscle found at front and side of abdomen. It is also paired. It attaches to ribs above and pelvic bones below. Its fibers run from the sides downwards like your hands tucked into jean pockets. Acting alone, the EAO rotates the torso; acting together EAO pulls chest toward pelvis (as in curl ups). It also compresses the abdominal cavity. This muscle is important for posture and torso movements.
Brachioradialis: red arrow- see above
Cephalic Vein: A vein of the arm – see below

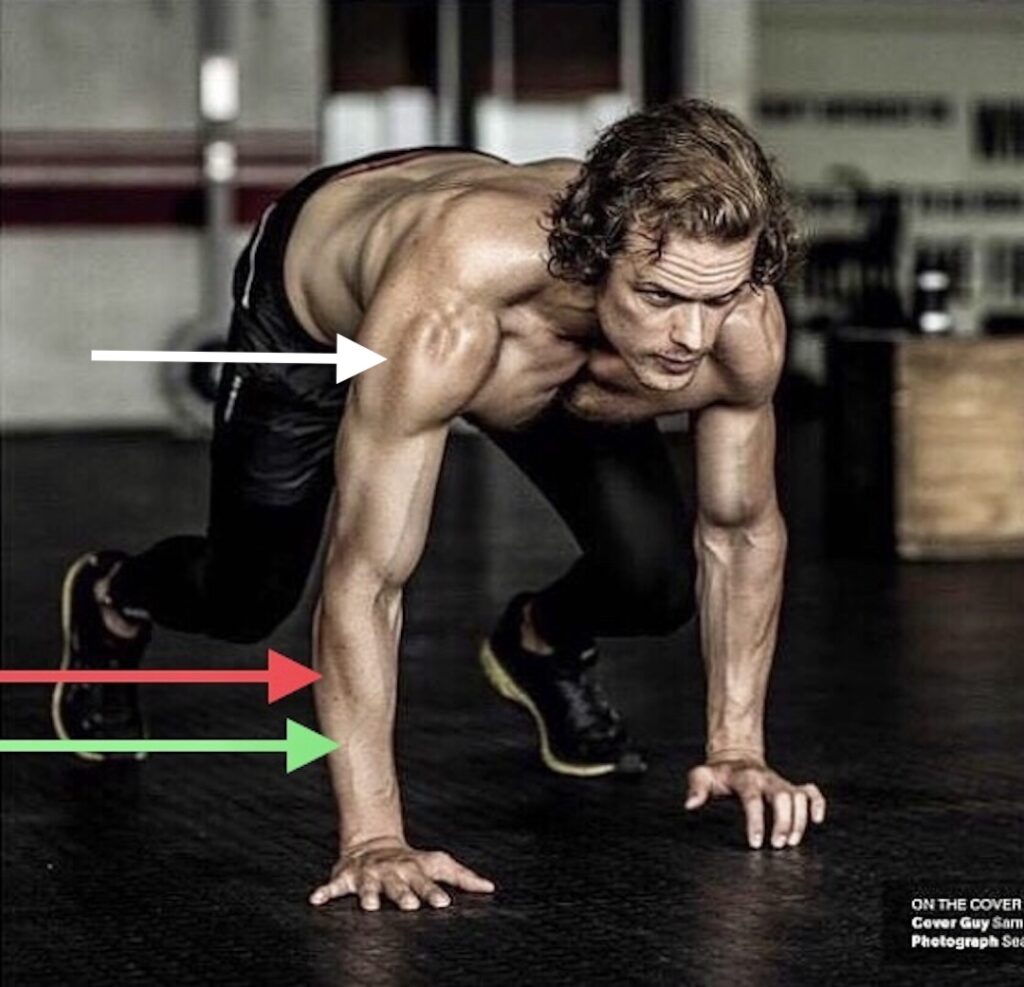
This image of Sam in a sprint position is awesome because it shows:
Posterior Deltoid: Already described above, the white arrow indicates the unusual and distinct groove between middle deltoid and posterior deltoid.
Extensor Digitorum: Green arrow – see above
Extensor Digiti Minimi: This wee muscle (red arrow) isn’t prominent unless the forearm is highly muscular and subcutaneous fat is low. EDM reaches from humerus to wee finger and extends (lifts) it.
Some X followers already have seen my tweet of this image of Michelangelo’s “Moses” sculpture. But, for those who haven’t, it shows the master’s attention to wee extensor digiti minimi! 🥰

Next is a full body view of Sam’s surface anatomy. This one shows a few arms veins that is a phlebotomist’s dream!
Just a note that venous pattern throughout the body is extremely varied so much so that hand vein patterns can be used to identify a person.
Median Antebrachial Vein: The median antebrachial vein (gold arrow) and its tributaries gather blood from hand and forearm and return it to the basilic vein (not shown).
Cephalic Vein: This large vein (red arrow) gathers blood from hand and forearm and returns it to a large vein (axillary vein) deep to the collar bone. Its name means “head” in Latin because its path through the arm points toward the head.
Deltopectoral Groove: Cephalic vein is traced through the deltopectoral groove (white arrow), a groove between anterior deltoid and pectoralis major muscles.
Median Cubital Vein: This vein (orange arrow) located in the cubital fossa (elbow hollow) forms a bridge connecting cephalic and basilic veins.
Fun Fact: Median cubital vein is the preferred site for blood draws because it is large and doesn’t tend to roll or move when a needle is inserted. The area also has fewer pain endings.
Moving to the lower limb! 🤗
Just So You Know: Anatomists define the thigh as that part of the lower limb between hip and knee and the part between knee and foot is the leg.
Vastus Lateralis: Aptly named, vastus lateralis (blue arrow) is vast on Sam-our-Man! Vastus lateralis is part of the quadraceps group of four (some say five) thigh muscles. It arises from the femur and inserts on the patella. It then joins the other quad tendons to form a common tendon that inserts on the tibia (largest leg bone). It is the largest and most powerful muscle of the quadraceps group. Together with the other quadraceps muscles, it extends (straightens) the knee joint and keeps patella in proper alignment.
Fun Fact: The vastus lateralis is the recommended site for intramuscular injection of infants under 7 months old and those unable to walk or with loss of muscle tone and mass.
Vastus Medialis: Also a member of quadraceps, this muscle (black arrow) arises from the femur and inserts on the patella and then, tibia. It has the same function as vastus medialis (see above).
Patella: Also known as the knee cap, patella (purple arrow) is the largest sesamoid bone in the body, meaning it is enclosed in ligament or tendon.
Gastrocnemius: Gastrocnemius has two heads arising from different parts of the femur. These join together to help form Achilles tendon which inserts into the calcaneus (heel bone). Sam’s medial head (green arrow) is very apparent in this image. It is a powerful muscle that plantar flexes (points) the foot and flexes the knee joint.
Tibia: Tibia (violet arrow) is also known as the shin bone. It is the larger of the two leg bones. Together with the femur, tibia forms the knee joint and with the fibula (smaller leg bone), it forms the ankle joint.

Next is a famous image of Sam flipping kilt for the “girls” at Emerald City ComicCon, March 6, 2017. Plenty of thigh muscle on display here! 😜
This amazing image is property of Marcia M Mueller. 👏🏻
Biceps Femoris: Biceps femoris (so named because it has two heads). The long head (red arrow) arises from the ischium (part of pelvic bone) and the short head (green arrow) arises from the femur (thigh bone). Both heads join into a single tendon that inserts on the fibula. Biceps femoris is a powerful flexor of the knee joint.
Not so Fun Fact: Avulsion (tearing away) of the biceps femoris tendon is common in sports that require explosive bending of the knee as seen with sprinting! 😱
Vastus Lateralis: Blue arrow – See above

Quiz time!
Try to identify the structures in this last image of Sam. Do your best. Answers appear after the image. Good luck!

-
- Orange arrow – sternocleidomastoid muscle
- Violet arrow – pectoralis major muscle
- Aqua arrow – Biceps brachii muscle
- Green arrow – Vastus lateralis muscle
- Red arrow – Vastus medialis muscle
- Blue arrow – medial head of gastrocnemius muscle
- White arrow – Inguinal groove, (aka Adonis belt) *** Extra credit for this one because we didn’t discuss! 😃
Well done, students! 🏆
The deeply grateful,
Outlander Anatomist
Follow me on:
-
- Twitter: @OutLandAnatomy
- Facebook: OutlandishAnatomyLessons
- Instagram: @outlanderanatomy
- Tumblr: @outlanderanatomy
- Youtube: Outlander Anatomy
Photo Creds: Sony/Starz; www.menshealth.com, www.thewrap.com, www.Wikimedia, @marciammueller, @samheughan, @kayzee














{kind=link}