
 Anatomy Def: Dupuytren’s Contracture, a disease involving changes to deep tissues of the palm.
Anatomy Def: Dupuytren’s Contracture, a disease involving changes to deep tissues of the palm.
Outlander Def: Tom Christie’s right hand enjoys Claire’s touch waaay too much. Watch out, Jamie! 😉
History: Dupuytren’s Contracture (DC) is named after Baron Guillaume Dupuytren (1777-1835), a French anatomist and military surgeon who gained considerable notoriety treating Napoleon Bonaparte’s hemorrhoids! 😲 Although he was not the first to recognize the condition, he was the first to perform a successful repair on DC and published the results (The Lancet, 1834). Hence, the disease is named for him.
Also Known As: Like Jamie, Dupuytren’s Contracture (DC) enjoys a number of aliases:
-
- Dupuytren’s disease (DD)
- Morbus Dupuytren
- Viking disease
- Celtic hand
- Palmar fibromatosis/familial palmar fibromatosis
- Palmar fascial fibromatosis.
Symptoms: Tight bands and/or firm lumps (nodules) appear in the tissues deep to the palmar skin. Gradually, the fingers may curl and pull sideways or toward the palm. Overlying skin may pucker. Sufferers may experience inflammation or sensations of tenderness, burning, or itching of the hand. Pressure or tension may be felt when attempting to straighten the fingers. Sometimes both hands and even the feet are affected. More fortunate individuals experience only mild cases that do not require medical intervention. The following image shows an example of DC involving the left ring finger.
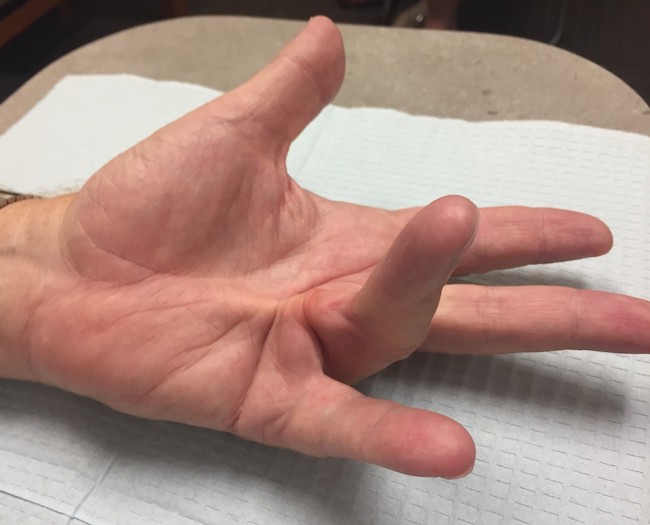
Diagnosis: Care givers use the tabletop test to help diagnose DC: the hand is placed palm-down on a flat surface. If DC is involved, the hand cannot be laid flat.

Now, onto the anatomy. Yay! 🤓
Try This: Look at your hand. Note that it has two main surfaces. The palm is known as the palmar surface; the back of the hand is its dorsal surface. See that the palmar skin is tightly adherent to underlying tissues, whereas the dorsal skin moves rather easily because it is loosely attached.
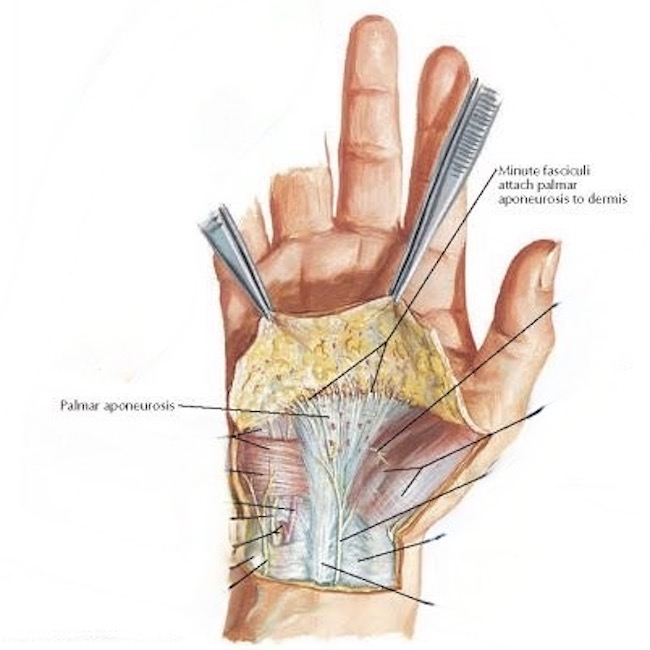
Palmar Aponeurosis: Deep to our palmar skin lies a thick fan-shaped layer of collagen known as the palmar fascia or, more formally, the palmar aponeurosis (next image). Collagen fibers (fasciculi) tightly bind the palmar skin to the underlying palmar aponeurosis. This anatomy enhances our grip, helps cup the palm, and protects underlying flexor tendons.
With the skin removed, the fan-shaped palmar aponeurosis is evident (next image): The point of the fan lies at the wrist (pink arrow), then it widens sending complex collagen bands to each of our four fingers (black arrows).
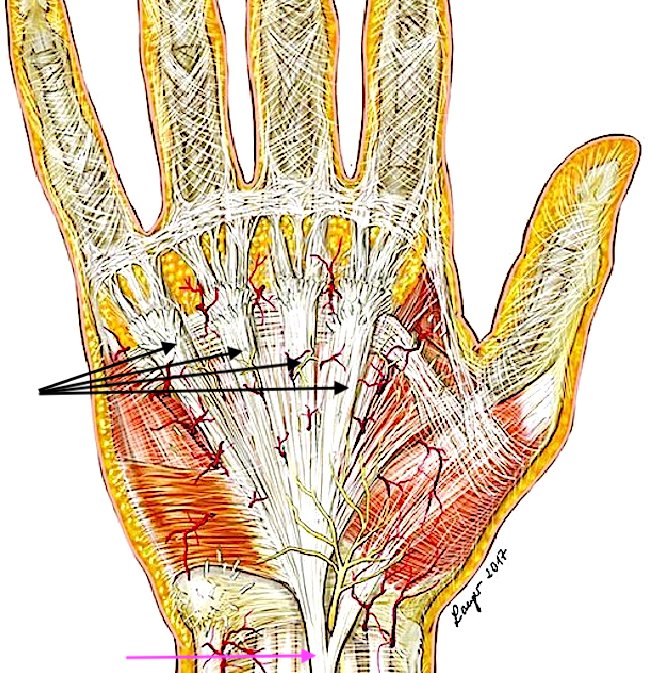
In case of DC, the long bands of collagen, along with some cross fibers, thicken, tighten, and may form nodules. Ring and little fingers are most commonly affected; thumb, and index and middle fingers are less often involved. Sometimes DC affects both hands and even the feet. Although some sources claim there is no correlation between occupation and development of this condition, others cite manual labor as a predisposing factor.
Learn more about the complex anatomy of the hand in Anatomy Lesson #22, Jamie’s Hand Symbol of Sacrifice and Anatomy Lesson #23, Harming Hands, Helping Hands, Healing Hands.
Cause: Although poorly understood, several parameters suggest DC is likely is an autoimmune disease caused by a single dominant gene which is unaffiliated with either X or Y chromosomes (the sex chromosomes). Even if present, the gene doesn’t always express itself. The reason for this is unknown.
Risk Factors: There are interesting risk factors associated with DC.
-
- Middle aged or older
- Male – much less common in females
- Scandinavian or Northern European descent (uncommon in Asian and African ethnicities)
- Family history
Other Associated Factors:
-
- Liver disease
- Long term use of phenytoin (anti-seizure med)
- Cigarette smoking
- Alcoholism
- Diabetes
- Nutritional deficiencies
Treatment of DC: For many years, surgery was the only treatment for DC. In recent times, this has changed and new strategies have appeared.
-
- Surgery: The most common treatment. Rarely, finger amputation is needed.
- Steroid injection: If a lump is painful, a steroid injection may help ease the pain. Repeated injections may be necessary.
- Radiation therapy: Low energy X-rays are directed at the nodules to soften them and reduce contractions. Uncommon treatment in the U.S.
- Enzyme injection: Newer, less invasive procedure. Hand is anesthetized, enzyme is injected. Over several hours, the enzyme breaks down and dissolves the tough bands.
- Needle aponeurotomy: Newer, less invasive procedure. Hand is anesthetized. Surgeon uses a needle to divide and release the diseased tissue.
Read about Tom’s disease in Diana’s sixth big book, “A Breath of Snow and Ashes.” Dr. Claire describes Tom’s suffering: 🤒
He had been suffering from a condition in the right hand called Dupuytren’s contracture—or at least it would be called that, once Baron Dupuytren got round to describing it in another sixty or seventy years. Caused by a thickening and shortening of the fibrous sheet that kept the hand’s tendons in place when the fingers flexed, the result of it was to draw the ring finger in toward the palm of the hand. In advanced cases, the little finger and sometimes the middle finger as well were involved. Tom Christie’s case had advanced quite a bit since I had last had the chance of a good look at his hand.
See Claire’s assessment of Tom Christie’s Dupuytren’s Contracture in Outlander episode 601, Echoes! Stay tuned! Claire will operate on Tom’s hand in Outlander Episode 603, “Temperance!” 😲
The deeply grateful,
Outlander Anatomist
Follow me on:
-
- Twitter: @OutLandAnatomy
- Facebook: OutlandishAnatomyLessons
- Instagram: @outlanderanatomy
- Tumblr: @outlanderanatomy
- Youtube: Outlander Anatomy
Photo Credits: Starz, www.johnericksonmd.com, Netter’s Atlas of Human Anatomy, www.OrthoBullets.com, www.researchgate.net
Eeep! I can’t look at some of those illustrations. I’ll leave it to the medical experts. 🙂 Thanks for explaining!
Sorry, Jordyn. Hope you can skip those and read the lesson. Lots of good info in there.
Wonderful analysis and information as always. Thank you!
Thank you so much, Margie, for reading and commenting. I am glad you found it interesting. All the best!
Just been diagnosed with this disease, so I’m pretty topical at the moment!
Hi Angela. Indeed, you are topical! I am glad you sought help. It is good to have a baseline assessment to determine if the condition worsens or remains the same.
I have heard from several women that they have received a DC diagnosis. I have also heard from several women that they have a mild case that has not increased in severity. I hope you will be in the latter cohort. All the best!
I’m thrilled to hear about the intimacy coach – especially as the couples and marriages age. Many of us could benefit from having our own intimacy coach! I would love to hear you describe the physical changes as we age; hormonal changes, vaginal dryness, hot flashes, erection disfunction, etc. Thank you for your dedication to making us all better informed and appreciative of our own bodies. Wish I had read “Our Bodies Ourselves” when it was first published in 1970! But it’s never too late to learn……
Dear Pat. It is never too late to learn. This is an interesting idea of yours. I have always awaited Outlander to supply me with the topic to address, but maybe I will prepare a lesson to address some of these aging topics. Let me think on it. Thank you for the brilliant ideas!
Hello Karmen: We’ve now gotten two examples of Claire experiencing symptoms of menopause. In 511 “The Journey” the script states that she is having a hot flash – so she gets out of bed and goes to the open window for some cool air. Great scene with Jaime holding her there so she can enjoy the night breeze!!
In 605 they are discussing “greased lightning” and “lubricating brilliance” – an obvious reference to enjoying sex with the aid of a lubricating oil. I hope its not lavender oil which might trigger Jamie into remembering BJR.
Thanks again for all of your great insights and comments!! Pat
Hi Pat. Yes, both could have been direct or indirect acknowledgement of menopause. ITB, Claire does use a cream on Jamie. The lubricated brilliance might be a nod to that part of the story. Thanks for your observations!
https://www.si.com/nfl/2019/08/22/john-elway-hand-disorder-dupuytrens-contracture-broncos
Thank you, Crystal. This was an interesting story. I am not a football fan so had not heard of John. I wish him all the best!
Is it also known as trigger finger ?
Thanks !
Wendy
Wendy! Hi! No. Trigger finger may sound similar because the finger can get caught in a bent position. However, the causes between it and Dupuytren’s are different. Trigger finger is due to inflammation of the sheath around a flexor tendon. Dupuytren’s is caused by thickening and tightening of the palmar aponeurosis which lies superficial to the flexor tendons. Good question. These two are frequently confused.
I’m glad to see this explanation…. I have been diagnosed with DC…just mild right now! Thanks for sharing your knowledge with us!
Hi Susie. Thank you for writing. I am glad you found the lesson helpful. I am also glad that you DC is mild. For some people, the disease never progresses. I hope you are in this category. Best of luck!
Love your lessons and commentary – fascinating and informative!
Thank you so much Debbie. I am glad it was useful for you!
Love the diagrams with arrows and labels. How about sharing with the Hudson Highlanders?🌞😜
Hi Susan
Thank you. Sure will. I had intended to anyway, but last night we did four Outlanderbts Zoom for three hours, so was work out by the time we were through!