
Anatomy Def: Claire confronts Dupuytren’s Contracture.
Outlander Def: A hand condition best dubbed as “Tom’s Travail!” 👋🏻
Tom’s right hand is disabled because he suffers from Dupuytren’s Contracture (DC). If you have not read my earlier Mini Anatomy Lesson about DC, you can access it here.
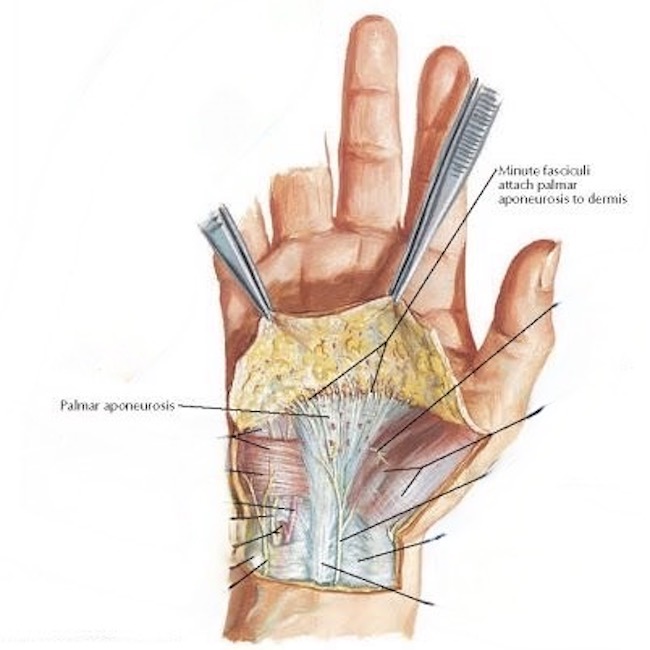
Quick Review: Underlying the skin of the palm is a tough layer of connective tissue known as the palmar aponeurosis. Importantly, it aids in cupping the palm, maintaining grip, and protecting underlying flexor tendons (see figure below).
DC causes the palmar aponeurosis to form thick bands and nodules that contract over time, typically drawing affected fingers toward the palm. Sometimes the palmar skin also contracts, scars, and pits.
What Claire Did: So, Claire says to Tom, “a stitch in time, saves nine.” She can fix what ails you, you auld sour pus.
Let’s do a quick recap of what Claire did. 🔪
First, and foremost, Claire kept Tom waiting. How dare you madam?

Tom’s at least as brave as Jamie so he’ll not be having any of yer potions, witchie Claire! If Jamie can stand it – so can Tom. (Jamie be like….hmmmm 🤔)

How about a wee stick to bite on ‘cos this WILL hurt! Nope, says Tom!
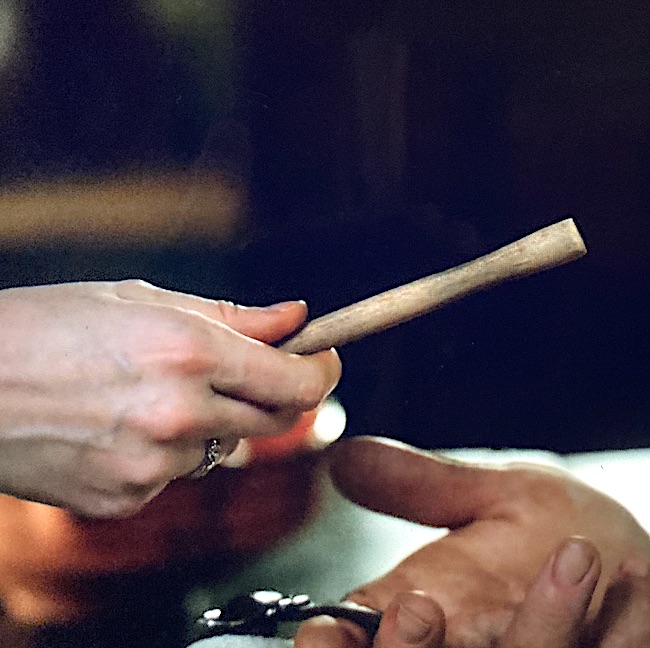
Alrightie, then….How about a big dram of whisky? Yep, says Tom! (Hey! It’s for medicinal purposes 🥃)

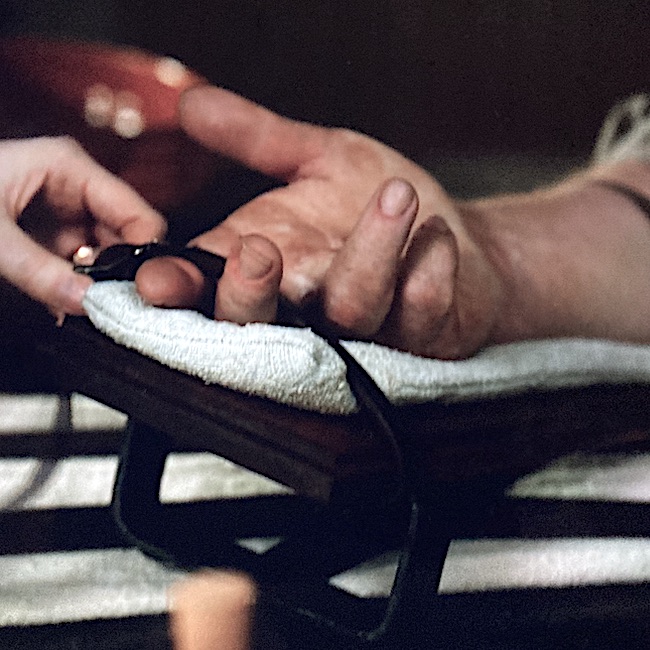
Claire buckles Tom’s hand to a nicely padded wee bed. Screaming is OK, but no move a muscle, Tom. Claire needs both hands to slice and dice. She canna be holding yours! 😷
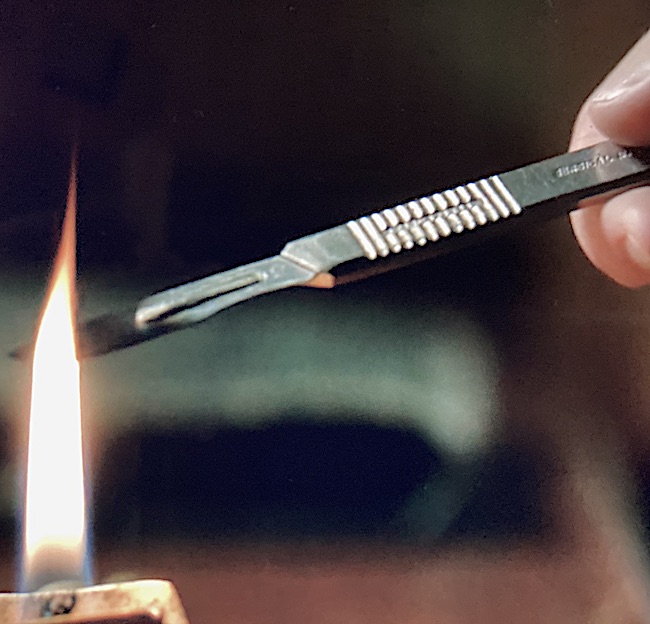
Claire’s wee alcohol lamp gleams, brightly!

Claire sterilizes her scalpel blade in the flame.
Erm, wait! Isn’t that a modern scalpel with a disposable blade and with info stamped in the handle? Ah…… yep.
Trouble is, knives with disposable blades weren’t invented until 1901 by King C. Gillette (yep, that Gillette), followed in 1906 by John Murphy, a surgeon who adapted Gillette’s razors into a surgical tool.
OK. Then, from whence did this scalpel come? I thought Claire’s medical kit perished back in Season 3 with the Artemis.
But, wait! She still wore her bat suit after washing ashore. Mayhap her med kit survived in one of its capacious pockets? If so, that blade may be a wee bit dull! 🤭
A chance to cut is a chance to cure! And, Doc Claire is off and running!
Claire makes a quick swipe of her scalpel across the palm of Tom’s hand.
@#%$&*! That HURTS!!!

Although that first transverse cut seems a wee bit deep and wide, let’s just accept the FX and move on. Aye?
Violet arrows point to the thick, tight bands of palmar aponeurosis that pull Tom’s fingers downward. Those must be cut away or divided.

Claire carefully makes zigzag cuts in the skin and frees it from the aponeurosis. She works to remove the thickened bands of connective tissue.

And, all the while, Jamie reads from Psalms at the back of Tom’s Bible. 😂 (Doesna matter, Jamie probs has all the psalms verses memorized anyhow.)
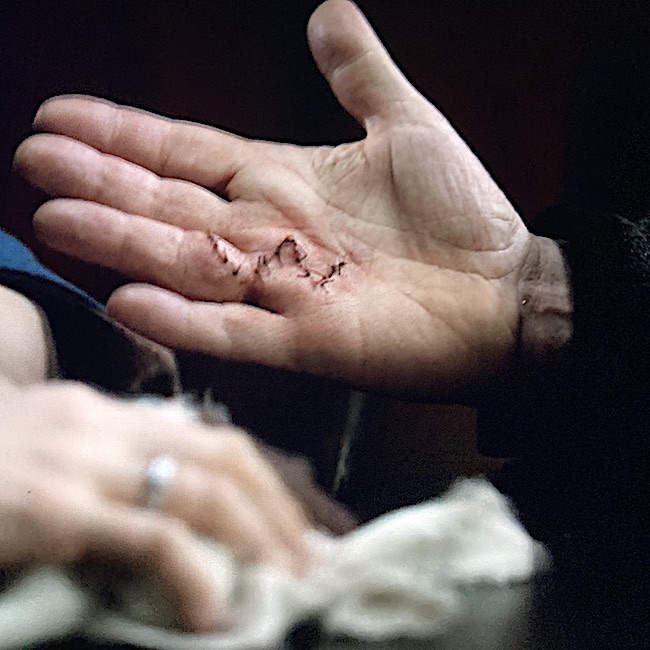
All done! A few snips and stitches later, the fingers are straight and the zig-zag opening is zippered shut. Tidy mending, Claire!

Hum…I understand that Tom’s Thumb and index were not a problem, but what about Tom’s wee finger, didn’t it have DC, too? 🧐
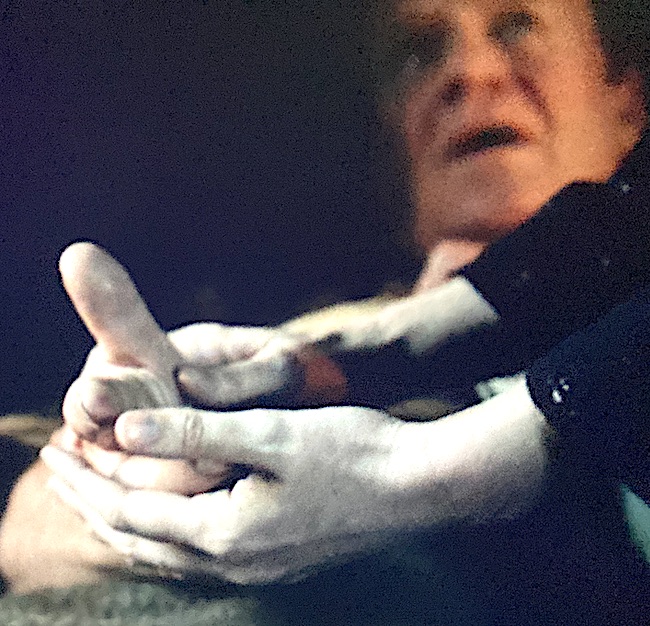
A few hours later, Claire offers Tom with some gentle PT. Tom has a fever so why not some penicillin?
Madam, you have a great deal too much hair!!!! Scary woman, why aren’t you a pious wife wearing a drab kerchief? 😈
So, how does Clair’s surgery compare to the real deal? Actually, pretty good.
WARNING: The following surgical images may be a bit graphic for some. If you are squeamish, you might wish to skip.
The following are five standard surgical approaches to DC:
-
- Regional Fasciectomy: Removal of the entire tight band(s) and/or nodule(s).
- Segmental fasciectomy: Removal of part of tight band(s) and/or nodule(s).
- Dermatofasciectomy: Removal of tight band plus overlying skin – requires a skin graft.
- Closed Fasciotomy: Dissection of the tight bands using needles. No skin incision. Available with patients who cannot tolerate fasciectomy.
- Finger Amputation: Amputation is employed in severe cases and after other approaches have failed.
BTW, fasciectomy means “to cut away fascia.” (Other names are fasciotomy and aponeurectomy).
It appears Claire performed a regional fasciectomy. Yay Claire! 🤜🏻🤛🏻
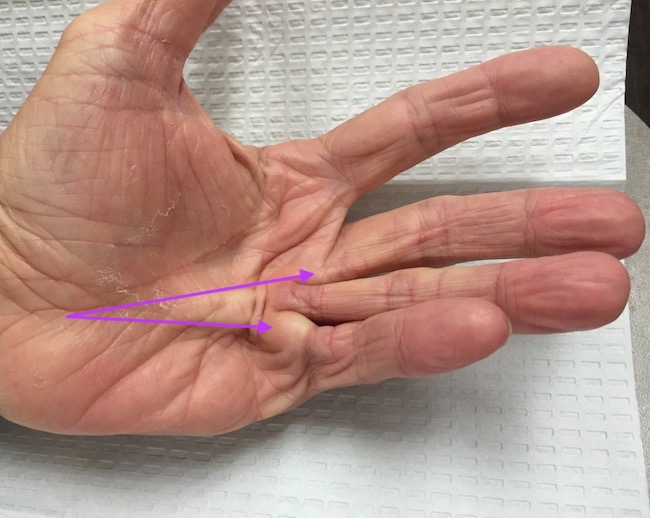
Now, let’s compare to a real surgery. The following image is a left hand with DC. A tight band extends into the middle finger (top arrow) and a nodule and band to the wee finger (bottom arrow). The ring finger appears less affected than middle and wee.
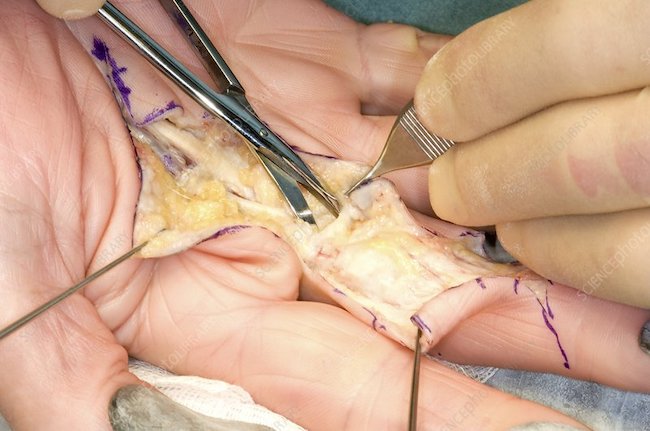
The surgeon opens the palmar skin to reveal the palmar aponeurosis. The tight bands are removed or split. Fine scissors and forceps are required to work carefully and meticulously to protect nearby neurovascular bundles and other important structures (next image).
Notice – the skin cuts are zigzags like Claire employed.
Why is this done?
ZigZag Cuts: ZZ cuts are employed for three good reasons:
-
- Scars from a straight line incision tend to contract more and may cause DC to recur early.
- Zigzag cuts mobilize more skin than a straight cut so the finger straightens better.
- Zigzag cuts rarely require skin grafting.
Lastly, thread tethers hold skin flaps out of the surgical field.
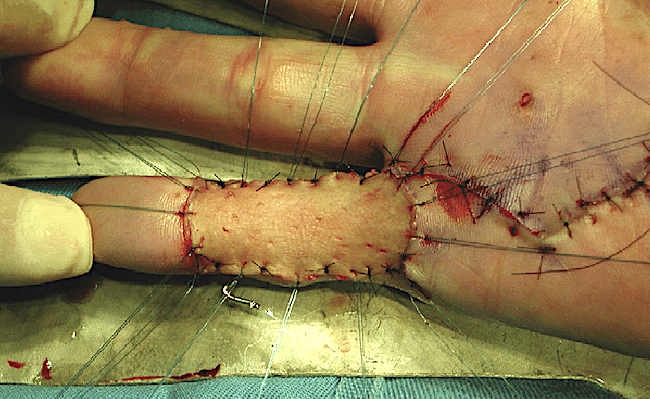
The next image shows a woman’s hand, post-surgery, wherein repairs were performed to middle, ring, and little fingers. The inked zigzags were drawn before surgery so the surgeon knows where to make the cuts. These are still visible, post-surgery.

Skin Graft: As mentioned above, If the overlying skin in DC is too damaged or it is not sufficient to close the surgical wound, a skin graft may be added; this permits the hand to be opened completely and laid flat (table top test). The follow image shows a skin graft of the little finger.
NOTE: Claire did not ink the intended zigzags on Tom’s palm although she had the means to do so. Also, the FX could have been improved by showing both ring and little finger repairs; only Tom’s ring finger showed Claire’s final handiwork. Over all, though, I thought the FX were good.
Genetics: Dupuytren’s Contracture, the most common of all connective tissue diseases, has a genetic basis. Two schools of thought explores the genetics of DC which runs in families and is more common in men and those of North European descent.
*Dominant Gene: This position claims DC is caused by a single dominant, non-sex-linked gene with incomplete penetrance. In common language:
-
- The person inherits only one DC gene from either parent.
- The gene is carried by a somatic chromosome – not X or Y.
- The gene may or may not expresses itself.
*Recessive Gene: This school of thought suggests the sufferer must inherit a recessive gene from each parent to get the disease. If (s)he receives just one recessive gene, then they are a DC carrier and do not have the disease.
Despite the prevalence of DC, its exact cause remain somewhat obscured.
So will all this cutting and stitching by Competent Claire fill Tom Christie with joy???? 🤔
The deeply grateful,
Outlander Anatomist
Follow me on:
-
- Twitter: @OutLandAnatomy
- Facebook: OutlandishAnatomyLessons
- Instagram: @outlanderanatomy
- Tumblr: @outlanderanatomy
- Youtube: Outlander Anatomy
Photo Credits: Starz, www.istockphoto.com, www.johnericksonmd.com, www.researchgate.com, www.sciencephoto.com